

Effect of treatment delay on the effectiveness and safety of antifibrinolytics in acute severe haemorrhage: a meta-analysis of individual patient-level data from 40 138 bleeding patients
- PMID: 29126600
- PMCID: PMC5773762
- DOI: 10.1016/S0140-6736(17)32455-8
Effect of treatment delay on the effectiveness and safety of antifibrinolytics in acute severe haemorrhage: a meta-analysis of individual patient-level data from 40 138 bleeding patients
Abstract
Background: Antifibrinolytics reduce death from bleeding in trauma and post-partum haemorrhage. We examined the effect of treatment delay on the effectiveness of antifibrinolytics.
Methods: We did an individual patient-level data meta-analysis of randomised trials done with more than 1000 patients that assessed antifibrinolytics in acute severe bleeding. We identified trials done between Jan 1, 1946, and April 7, 2017, from MEDLINE, Embase, the Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, PubMed, Popline, and the WHO International Clinical Trials Registry Platform. The primary measure of treatment benefit was absence of death from bleeding. We examined the effect of treatment delay on treatment effectiveness using logistic regression models. We investigated the effect of measurement error (misclassification) in sensitivity analyses. This study is registered with PROSPERO, number 42016052155.
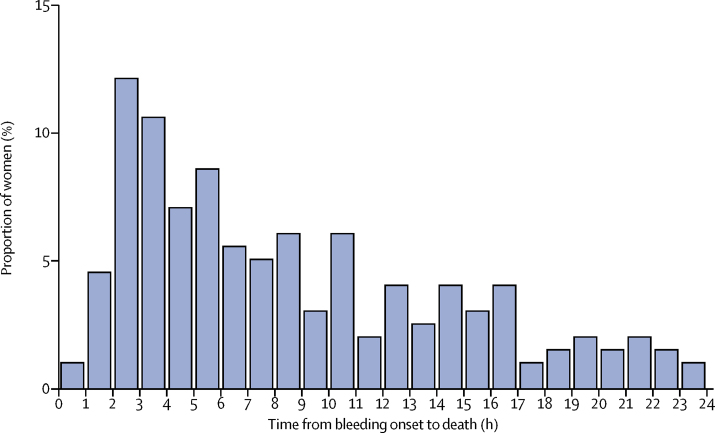
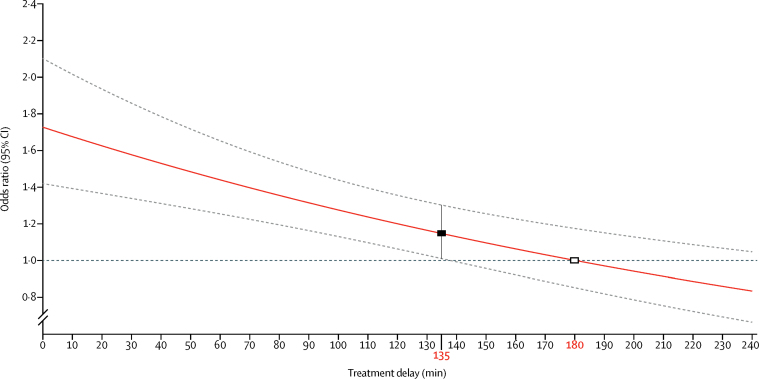
Findings: We obtained data for 40 138 patients from two randomised trials of tranexamic acid in acute severe bleeding (traumatic and post-partum haemorrhage). Overall, there were 3558 deaths, of which 1408 (40%) were from bleeding. Most (884 [63%] of 1408) bleeding deaths occurred within 12 h of onset. Deaths from post-partum haemorrhage peaked 2-3 h after childbirth. Tranexamic acid significantly increased overall survival from bleeding (odds ratio [OR] 1·20, 95% CI 1·08-1·33; p=0·001), with no heterogeneity by site of bleeding (interaction p=0·7243). Treatment delay reduced the treatment benefit (p<0·0001). Immediate treatment improved survival by more than 70% (OR 1·72, 95% CI 1·42-2·10; p<0·0001). Thereafter, the survival benefit decreased by 10% for every 15 min of treatment delay until 3 h, after which there was no benefit. There was no increase in vascular occlusive events with tranexamic acid, with no heterogeneity by site of bleeding (p=0·5956). Treatment delay did not modify the effect of tranexamic acid on vascular occlusive events.
Interpretation: Death from bleeding occurs soon after onset and even a short delay in treatment reduces the benefit of tranexamic acid administration. Patients must be treated immediately. Further research is needed to deepen our understanding of the mechanism of action of tranexamic acid.
Funding: UK NIHR Health Technology Assessment programme, Pfizer, BUPA Foundation, and J P Moulton Charitable Foundation (CRASH-2 trial). London School of Hygiene & Tropical Medicine, Pfizer, UK Department of Health, Wellcome Trust, and Bill & Melinda Gates Foundation (WOMAN trial).
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC-BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures


Comment in
-
Tranexamic acid: is it about time?Lancet. 2018 Jan 13;391(10116):97-98. doi: 10.1016/S0140-6736(17)32806-4. Epub 2017 Nov 7. Lancet. 2018. PMID: 29126598 No abstract available.
-
Effect of treatment delay on the effectiveness and safety of antifibrinolytics in acute severe hemorrhage.J Thromb Haemost. 2018 Jun;16(6):1025-1027. doi: 10.1111/jth.14010. Epub 2018 May 24. J Thromb Haemost. 2018. PMID: 29797789 No abstract available.
References
-
- Bruns J, Hauser W. The epidemiology of traumatic brain injury: a review. Epilepsia. 2003;44(suppl 10):2–10. - PubMed
-
- Karkouki K, Wijeysundera DN, Yau TM. The independent association of massive blood loss with mortality in cardiac surgery. Transfusion. 2004;44:1453–1462. - PubMed
-
- Hearnshaw SA, Logan RF, Lowe D, Travis SP, Murphy MF, Palmer KR. Acute upper gastrointestinal bleeding in the UK: patients characteristics, diagnoses and outcomes in the 2007 UK audit. Gut. 2011;60:1327–1335. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
