

Effect of Adding Dexamethasone to Continued Ranibizumab Treatment in Patients With Persistent Diabetic Macular Edema: A DRCR Network Phase 2 Randomized Clinical Trial
- PMID: 29127949
- PMCID: PMC5833605
- DOI: 10.1001/jamaophthalmol.2017.4914
Effect of Adding Dexamethasone to Continued Ranibizumab Treatment in Patients With Persistent Diabetic Macular Edema: A DRCR Network Phase 2 Randomized Clinical Trial
Abstract
Importance: Some eyes have persistent diabetic macular edema (DME) following anti-vascular endothelial growth factor (anti-VEGF) therapy for DME. Subsequently adding intravitreous corticosteroids to the treatment regimen might result in better outcomes than continued anti-VEGF therapy alone.
Objective: To compare continued intravitreous ranibizumab alone with ranibizumab plus intravitreous dexamethasone implant in eyes with persistent DME.
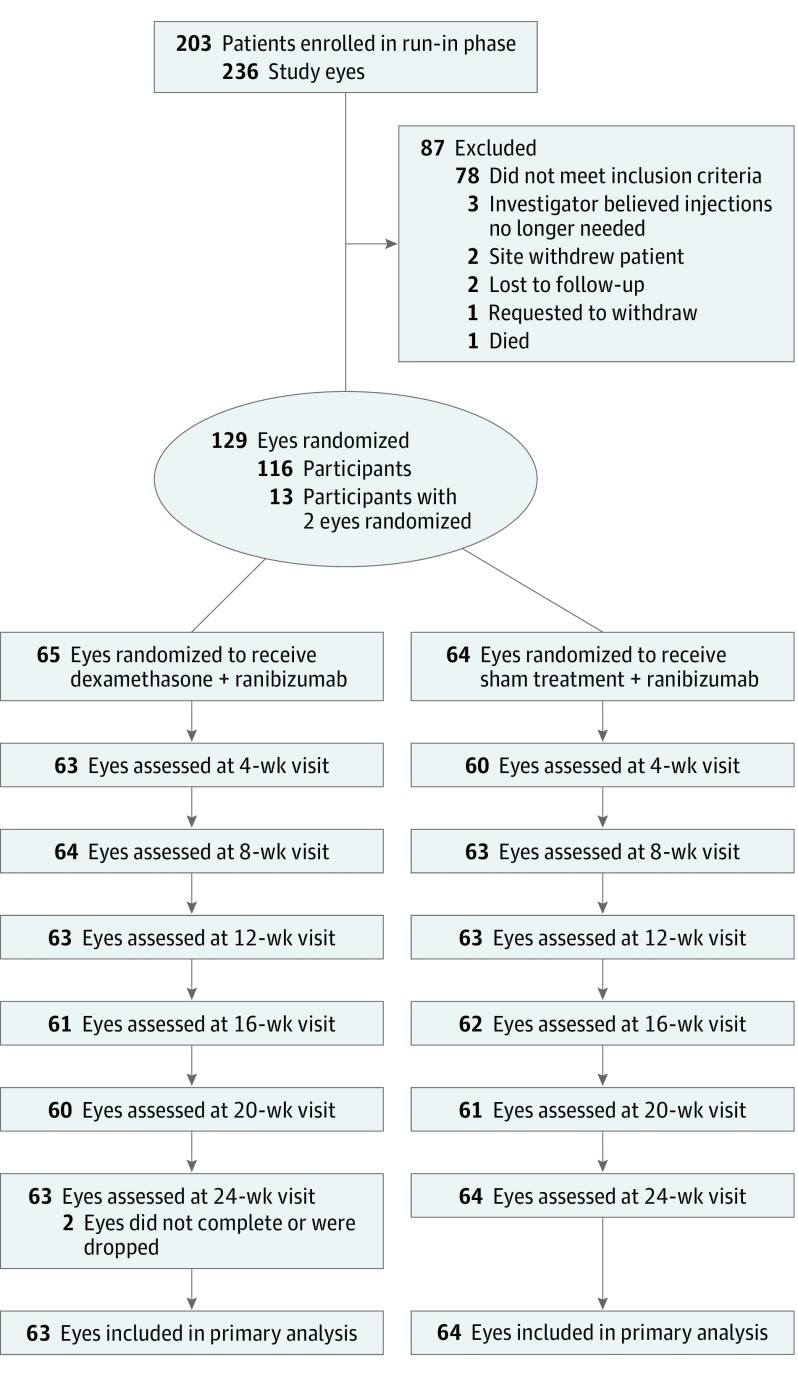
Design, setting, and participants: Phase 2 multicenter randomized clinical trial conducted at 40 US sites in 129 eyes from 116 adults with diabetes between February 2014 and December 2016. Eyes had persistent DME, with visual acuity of 20/32 to 20/320 after at least 3 anti-VEGF injections before a run-in phase, which included an additional 3 monthly 0.3-mg ranibizumab injections. Data analysis was according to intent to treat.
Interventions: Following the run-in phase, study eyes that had persistent DME and were otherwise eligible were randomly assigned to receive 700 μg of dexamethasone (combination group, 65 eyes) or sham treatment (ranibizumab group, 64 eyes) in addition to continued 0.3-mg ranibizumab in both treatment arms as often as every 4 weeks based on a structured re-treatment protocol.
Main outcomes and measures: The primary outcome was change in mean visual acuity letter score at 24 weeks as measured by the electronic Early Treatment Diabetic Retinopathy Study (E-ETDRS). The principal secondary outcome was change in mean central subfield thickness as measured with the use of optical coherence tomography.
Results: Of the 116 randomized patients, median age was 65 years (interquartile range [IQR], 58-71 years); 50.9% were female and 60.3% were white. Mean (SD) improvement in visual acuity from randomization was 2.7 (9.8) letters in the combination group and 3.0 (7.1) letters in the ranibizumab group, with the adjusted treatment group difference (combination minus ranibizumab) of -0.5 letters (95% CI, -3.6 to 2.5; 2-sided P = .73). Mean (SD) change in central subfield thickness in the combination group was -110 (86) μm compared with -62 (97) μm for the ranibizumab group (adjusted difference, -52; 95% CI, -82 to -22; 2-sided P < .001). Nineteen eyes (29%) in the combination group experienced increased intraocular pressure or initiated treatment with antihypertensive eyedrops compared with 0 in the ranibizumab group (2-sided P < .001).
Conclusions and relevance: Although its use is more likely to reduce retinal thickness and increase intraocular pressure, the addition of intravitreous dexamethasone to continued ranibizumab therapy does not improve visual acuity at 24 weeks more than continued ranibizumab therapy alone among eyes with persistent DME following anti-VEGF therapy.
Trial registration: clinicaltrials.gov Identifier: NCT01945866.
Conflict of interest statement
Figures

References
-
- Nguyen QD, Brown DM, Marcus DM, et al. ; RISE and RIDE Research Group . Ranibizumab for diabetic macular edema: results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology. 2012;119(4):789-801. - PubMed
-
- Mitchell P, Bandello F, Schmidt-Erfurth U, et al. ; RESTORE Study Group . The RESTORE study: ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology. 2011;118(4):615-625. - PubMed
-
- Nauck M, Karakiulakis G, Perruchoud AP, Papakonstantinou E, Roth M. Corticosteroids inhibit the expression of the vascular endothelial growth factor gene in human vascular smooth muscle cells. Eur J Pharmacol. 1998;341(2-3):309-315. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
