

Temporal trends and hospital-level variation of inhospital cardiac arrest incidence and outcomes in the Veterans Health Administration
- PMID: 29129250
- PMCID: PMC6312852
- DOI: 10.1016/j.ahj.2017.05.018
Temporal trends and hospital-level variation of inhospital cardiac arrest incidence and outcomes in the Veterans Health Administration
Abstract
Background: Despite significant attention to resuscitation care by hospitals, national data on trends in the incidence and survival of patients with inhospital cardiac arrest (IHCA) are limited.
Objective: To determine trends and hospital-level variation in the incidence and outcomes associated with IHCA. In exploratory analyses, we evaluated the relationship between hospital-level IHCA incidence and outcomes with general hospital-wide quality improvement activities.
Design, setting, and participants: Retrospective cohort study of 2,205,123 hospitalizations at 101 Veterans Health Administration (VHA) hospitals between 2008 and 2012.
Main outcomes: Risk- and reliability-adjusted hospital-level IHCA incidence and survival to hospital discharge.
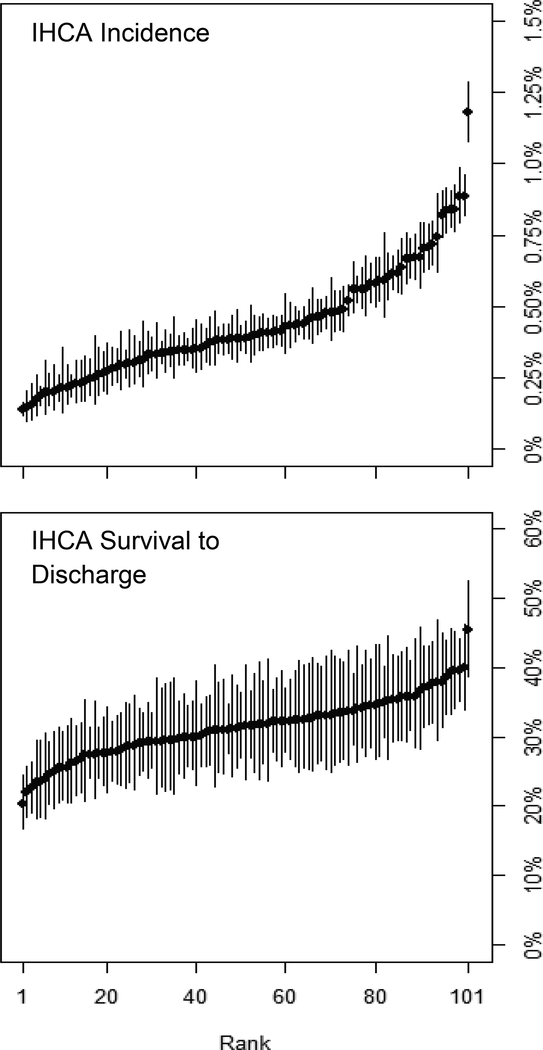
Results: A total of 8821 (0.40%) IHCA occurred between 2008 and 2012, with no significant change in risk-adjusted incidence over this time (P = .77). Hospital-level IHCA incidence varied substantially across facilities, with a median hospital incidence of 4.0 per 1000 hospitalizations and a range from 1.4 to 11.8 per 1000 hospitalizations. Overall, survival to discharge after IHCA was 31.2%. Risk-adjusted odds of survival increased over the study period (2012 vs 2008, OR: 1.49, 95% CI: 1.27, 1.75) but survival varied substantially across facilities from 20.3% to 45.4%. General hospital quality improvement activities were inconsistently associated with IHCA incidence and survival.
Conclusions: Within the VHA, the incidence and outcomes of IHCA showed important trends over time but varied substantially across hospitals with no consistent link to general hospital quality improvement activities. Identification of specific resuscitation practices at hospitals with low incidence and high survival of IHCA may guide further improvements for inhospital resuscitation.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
-
- Gage H, Kenward G, Hodgetts TJ, Castle N, Ineson N, Shaikh L. Health system costs of in-hospital cardiac arrest. Resuscitation. 2002;54(2):139–146. - PubMed
-
- Paniagua D, Lopez-Jimenez F, Londoño JC, Mangione CM, Fleischmann K, Lamas GA. Outcome and cost-effectiveness of cardiopulmonary resuscitation after in-hospital cardiac arrest in octogenarians. Cardiology. 2002;97(1):6–11. doi:47412. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
