

Evaluation of ECG algorithms designed to improve detect of transient myocardial ischemia to minimize false alarms in patients with suspected acute coronary syndrome
- PMID: 29129350
- PMCID: PMC5845470
- DOI: 10.1016/j.jelectrocard.2017.10.005
Evaluation of ECG algorithms designed to improve detect of transient myocardial ischemia to minimize false alarms in patients with suspected acute coronary syndrome
Abstract
Background: Patients hospitalized for suspected acute coronary syndrome (ACS) are at risk for transient myocardial ischemia. During the "rule-out" phase, continuous ECG ST-segment monitoring can identify transient myocardial ischemia, even when asymptomatic. However, current ST-segment monitoring software is vastly underutilized due to false positive alarms, with resultant alarm fatigue. Current ST algorithms may contribute to alarm fatigue because; (1) they are not designed with a delay (minutes), rather alarm to brief spikes (i.e., turning, heart rate changes), and (2) alarm to changes in a single ECG lead, rather than contiguous leads.
Purpose: This study was designed to determine sensitivity, and specificity, of ST algorithms when accounting for; ST magnitude (100μV vs 200μV), duration, and changes in contiguous ECG leads (i.e., aVL, I, - aVR, II, aVF, III; V1, V2, V3, V4, V5, V6, V6, I).
Methods: This was a secondary analysis from the COMPARE Study, which assessed occurrence rates for transient myocardial ischemia in hospitalized patients with suspected ACS using 12-lead Holter. Transient myocardial ischemia was identified from Holter using >100μV ST-segment ↑ or ↓, in >1 ECG lead, >1min. Algorithms tested against Holter transient myocardial ischemia were done using the University of California San Francisco (UCSF) ECG algorithm and included: (1)100μV vs 200μV any lead during a 5-min ST average; (2)100μV vs 200μV any lead >5min, (3) 100μV vs 200μV any lead during a 5-min ST average in contiguous leads, and (4) 100μV vs 200μV>5min in contiguous leads (Table below).
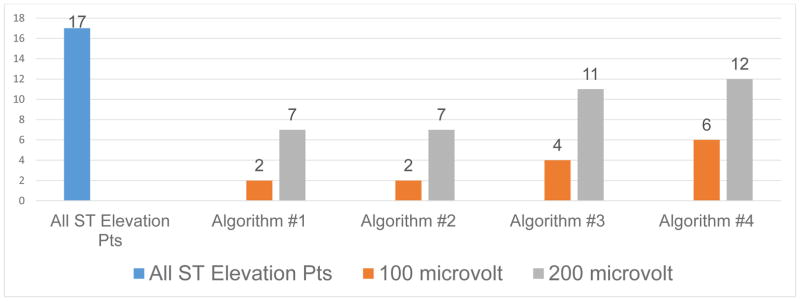
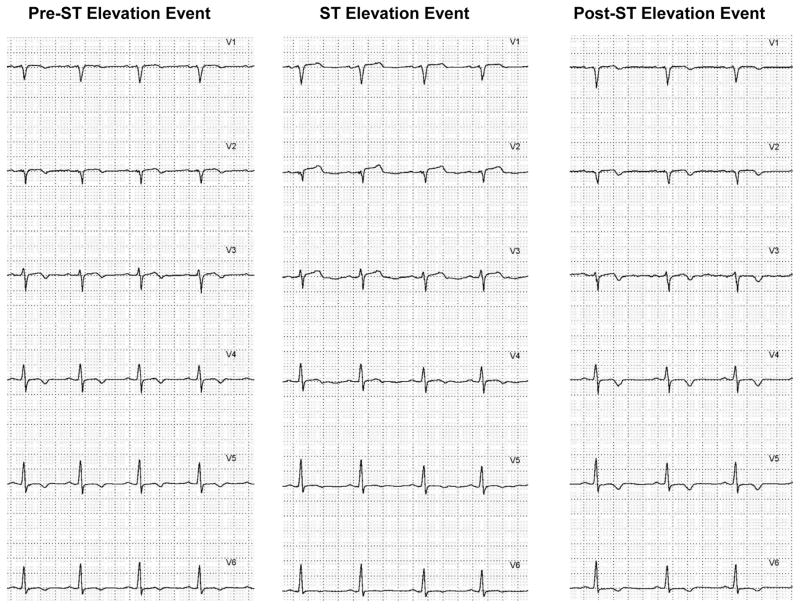
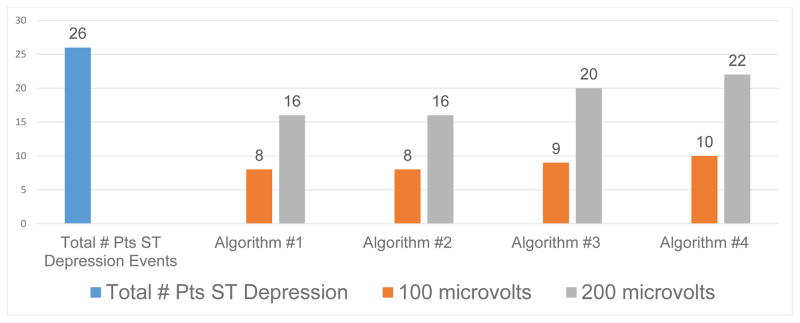
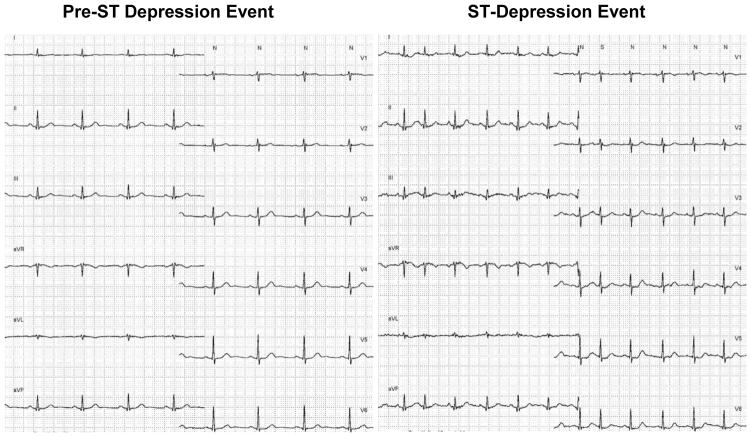
Results: In 361 patients; mean age 63+12years, 63% male, 56% prior CAD, 43 (11%) had transient myocardial ischemia. Of the 43 patients with transient myocardial ischemia, 17 (40%) had ST-segment elevation events, and 26 (60%) ST-segment depression events. A higher proportion of patients with ST segment depression has missed ischemic events. Table shows sensitivity and specificity for the four algorithms tested.
Conclusions: Sensitivity was highly variable, due to the ST threshold selected, with the 100μV measurement point being superior to the 200μV amplitude threshold. Of all the algorithms tested, there was moderate sensitivity and specificity (70% and 68%) using the 100μV ST-segment threshold, integrated ST-segment changes in contiguous leads during a 5-min average.
Keywords: Acute Coronary Syndrome; Algorithm Development; Hospital ECG Monitoring; Myocardial Ischemia; ST Monitoring.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest: none
Figures
Similar articles
-
Criteria for ECG detection of acute myocardial ischemia: Sensitivity versus specificity.J Electrocardiol. 2018 Nov-Dec;51(6S):S12-S17. doi: 10.1016/j.jelectrocard.2018.08.018. Epub 2018 Aug 13. J Electrocardiol. 2018. PMID: 30177366
-
A research method for detecting transient myocardial ischemia in patients with suspected acute coronary syndrome using continuous ST-segment analysis.J Vis Exp. 2012 Dec 28;(70):50124. doi: 10.3791/50124. J Vis Exp. 2012. PMID: 23299490 Free PMC article.
-
Unplanned transfer from the telemetry unit to the intensive care unit in hospitalized patients with suspected acute coronary syndrome.J Electrocardiol. 2016 Nov-Dec;49(6):775-783. doi: 10.1016/j.jelectrocard.2016.08.010. Epub 2016 Aug 26. J Electrocardiol. 2016. PMID: 27623400 Free PMC article.
-
The 24-lead ECG display for enhanced recognition of STEMI-equivalent patterns in the 12-lead ECG.J Electrocardiol. 2014 Jul-Aug;47(4):425-9. doi: 10.1016/j.jelectrocard.2014.04.007. Epub 2014 Apr 18. J Electrocardiol. 2014. PMID: 24880763 Review.
-
Electrocardiogram patterns in acute left main coronary artery occlusion.J Electrocardiol. 2008 Nov-Dec;41(6):626-9. doi: 10.1016/j.jelectrocard.2008.06.020. Epub 2008 Sep 13. J Electrocardiol. 2008. PMID: 18790498 Review.
Cited by
-
Meta-Analysis of Dynamic Electrocardiography in the Diagnosis of Myocardial Ischemic Attack of Coronary Heart Disease.Comput Math Methods Med. 2022 Jun 7;2022:3472413. doi: 10.1155/2022/3472413. eCollection 2022. Comput Math Methods Med. 2022. Retraction in: Comput Math Methods Med. 2023 Jun 28;2023:9838452. doi: 10.1155/2023/9838452. PMID: 35712003 Free PMC article. Retracted.
-
Occurrence of Transient Myocardial Ischemic Events Among Non-ST Segment Elevation Acute Coronary Syndrome Patients Before or After Invasive Coronary Angiography.Crit Pathw Cardiol. 2024 Sep 1;23(3):131-136. doi: 10.1097/HPC.0000000000000356. Epub 2024 Apr 5. Crit Pathw Cardiol. 2024. PMID: 38578970
-
Predictive Value of Serial ECGs in Patients with Suspected Myocardial Infarction.J Clin Med. 2020 Jul 20;9(7):2303. doi: 10.3390/jcm9072303. J Clin Med. 2020. PMID: 32698466 Free PMC article.
-
Monitoring significant ST changes through deep learning.J Electrocardiol. 2018 Nov-Dec;51(6S):S78-S82. doi: 10.1016/j.jelectrocard.2018.07.026. Epub 2018 Aug 1. J Electrocardiol. 2018. PMID: 30082087 Free PMC article. No abstract available.
References
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jiménez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P. Heart Disease and Stroke Statistics—2017 Update: A Report From the American Heart Association. Circulation. 2017 - PMC - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Jr, Ganiats TG, Holmes DR, Jr, Jaffe AS, Jneid H, Kelly RF, Kontos MC, Levine GN, Liebson PR, Mukherjee D, Peterson ED, Sabatine MS, Smalling RW, Zieman SJ C. American College of, G. American Heart Association Task Force on Practice, A. Society for Cardiovascular, Interventions, S. Society of Thoracic, and C. American Association for Clinical 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139–228. - PubMed
-
- Drew BJ, Pelter MM, Adams MG. Frequency, characteristics, and clinical significance of transient ST segment elevation in patients with acute coronary syndromes. Eur Heart J. 2002;23(12):941–7. - PubMed
-
- Pelter MM, Loranger DL, Kozik TM, Kedia A, Ganchan RP, Ganchan D, Hu X, Carey MG. Among Unstable Angina and Non-ST-Elevation Myocardial Infarction Patients, Transient Myocardial Ischemia and Early Invasive Treatment Are Predictors of Major In-hospital Complications. J Cardiovasc Nurs. 2016;31(4):E10–9. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
