

Cardiometabolic outcomes and mortality in medically treated primary aldosteronism: a retrospective cohort study
- PMID: 29129576
- PMCID: PMC5953512
- DOI: 10.1016/S2213-8587(17)30367-4
Cardiometabolic outcomes and mortality in medically treated primary aldosteronism: a retrospective cohort study
Abstract
Background: Mineralocorticoid receptor (MR) antagonists are the recommended medical therapy for primary aldosteronism. Whether this recommendation effectively reduces cardiometabolic risk is not well understood. We aimed to investigate the risk of incident cardiovascular events in patients with primary aldosteronism treated with MR antagonists compared with patients with essential hypertension.
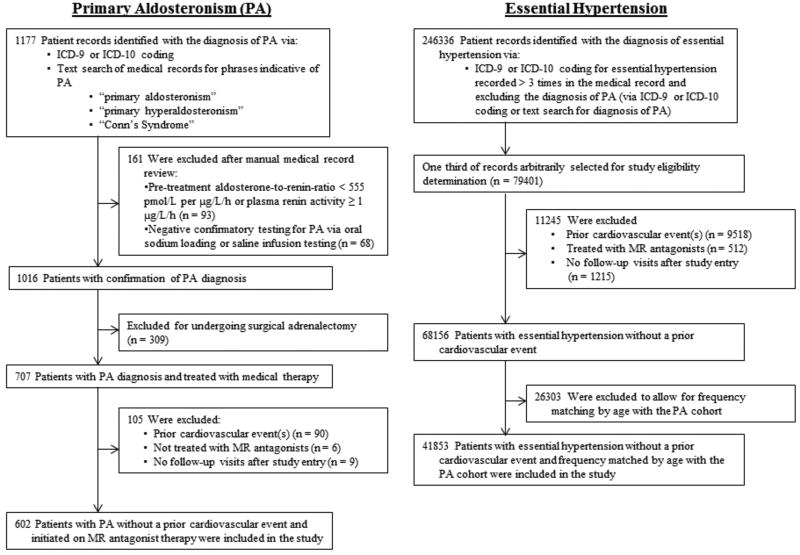
Methods: We did a cohort study using patients from a research registry from Brigham and Women's Hospital, Massachusetts General Hospital, and their affiliated partner hospitals. We identified patients with primary aldosteronism using International Classification of Disease, 9th and 10th Revision codes, who were assessed between the years 1991-2016 and were at least 18 years of age. We excluded patients who underwent surgical adrenalectomy, had a previous cardiovascular event, were not treated with MR antagonists, or had no follow-up visits after study entry. From the same registry, we identified a population with essential hypertension that was frequency matched by decade of age at study entry. We extracted patient cohort data and collated it into a de-identified database. The primary outcome was an incident cardiovascular event, defined as a composite of incident myocardial infarction or coronary revascularisation, hospital admission with congestive heart failure, or stroke, which was assessed using adjusted Cox regression models. Secondary outcomes were the individual components of the composite cardiovascular outcome, as well as incident atrial fibrillation, incident diabetes, and death.
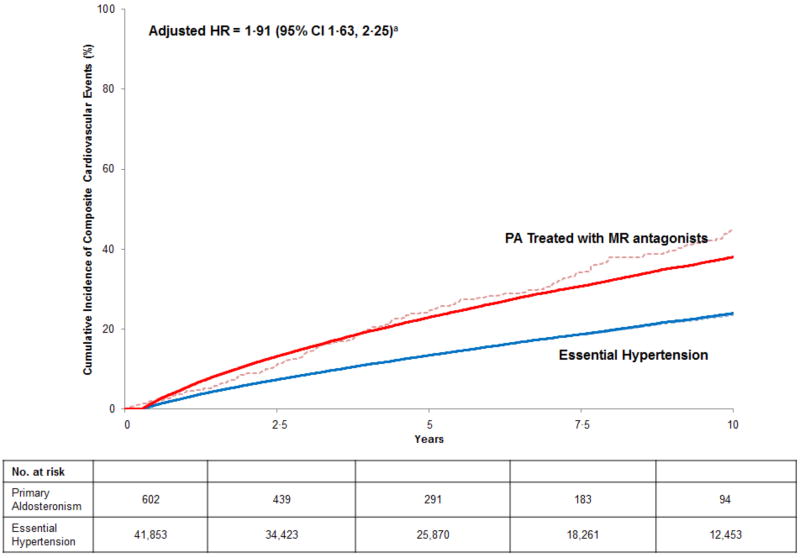
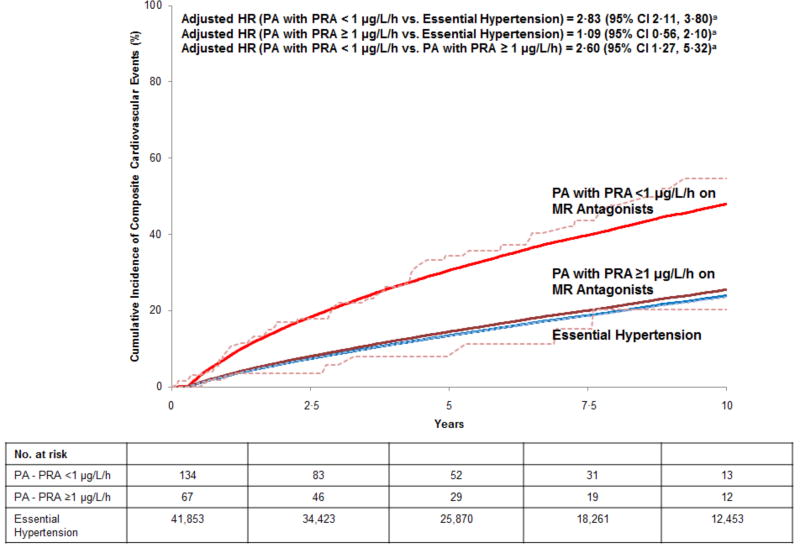
Findings: We identified 602 eligible patients with primary aldosteronism treated with MR antagonists and 41 853 age-matched patients with essential hypertension from the registry. The two groups of patients had comparable cardiovascular risk profiles and blood pressure throughout the study. The incidence of cardiovascular events was higher in patients with primary aldosteronism on MR antagonists than in patients with essential hypertension (56·3 [95% CI 48·8-64·7] vs 26·6 [26·1-27·2] events per 1000 person-years, adjusted hazard ratio 1·91 [95% CI 1·63-2·25]; adjusted 10-year cumulative incidence difference 14·1 [95% CI 10·1-18·0] excess events per 100 people). Patients with primary aldosteronism also had higher adjusted risks for incident mortality (hazard ratio [HR] 1·34 [95% CI 1·06-1·71]), diabetes (1·26 [1·01-1·57]), and atrial fibrillation (1·93 [1·54-2·42]). Compared with essential hypertension, the excess risk for cardiovascular events and mortality was limited to patients with primary aldosteronism whose renin activity remained suppressed (<1 μg/L per h) on MR antagonists (adjusted HR [2·83 [95% CI 2·11-3·80], and 1·79 [1·14-2·80], respectively) whereas patients who were treated with higher MR antagonist doses and had unsuppressed renin (≥1 μg/L per h) had no significant excess risk.
Interpretation: The current practice of MR antagonist therapy in primary aldosteronism is associated with significantly higher risk for incident cardiometabolic events and death, independent of blood pressure control, than for patients with essential hypertension. Titration of MR antagonist therapy to raise renin might mitigate this excess risk.
Funding: US National Institutes of Health.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
All authors declare no competing interests.
Figures
References
-
- Conn JW. Plasma Renin Activity in Primary Aldosteronism. Importance in Differential Diagnosis and in Research of Essential Hypertension. JAMA. 1964;190:222–5. - PubMed
-
- Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, Stowasser M, Young WF., Jr The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(5):1889–916. - PubMed
-
- Monticone S, Burrello J, Tizzani D, Bertello C, Viola A, Buffolo F, Gabetti L, Mengozzi G, Williams TA, Rabbia F, Veglio F, Mulatero P. Prevalence and Clinical Manifestations of Primary Aldosteronism Encountered in Primary Care Practice. J Am Coll Cardiol. 2017;69(14):1811–20. - PubMed
-
- Piaditis G, Markou A, Papanastasiou L, Androulakis II, Kaltsas G. Progress in aldosteronism: a review of the prevalence of primary aldosteronism in pre-hypertension and hypertension. Eur J Endocrinol. 2015;172(5):R191–203. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
