

Mechanisms by which a Very-Low-Calorie Diet Reverses Hyperglycemia in a Rat Model of Type 2 Diabetes
- PMID: 29129786
- PMCID: PMC5762419
- DOI: 10.1016/j.cmet.2017.10.004
Mechanisms by which a Very-Low-Calorie Diet Reverses Hyperglycemia in a Rat Model of Type 2 Diabetes
Abstract
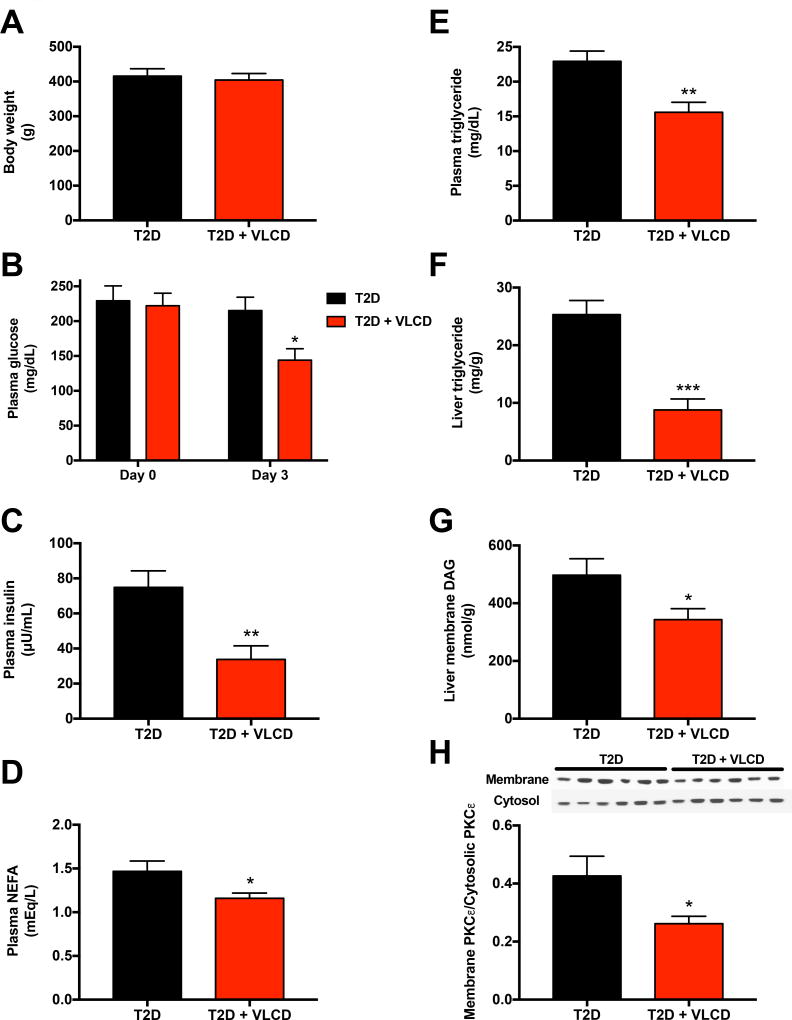
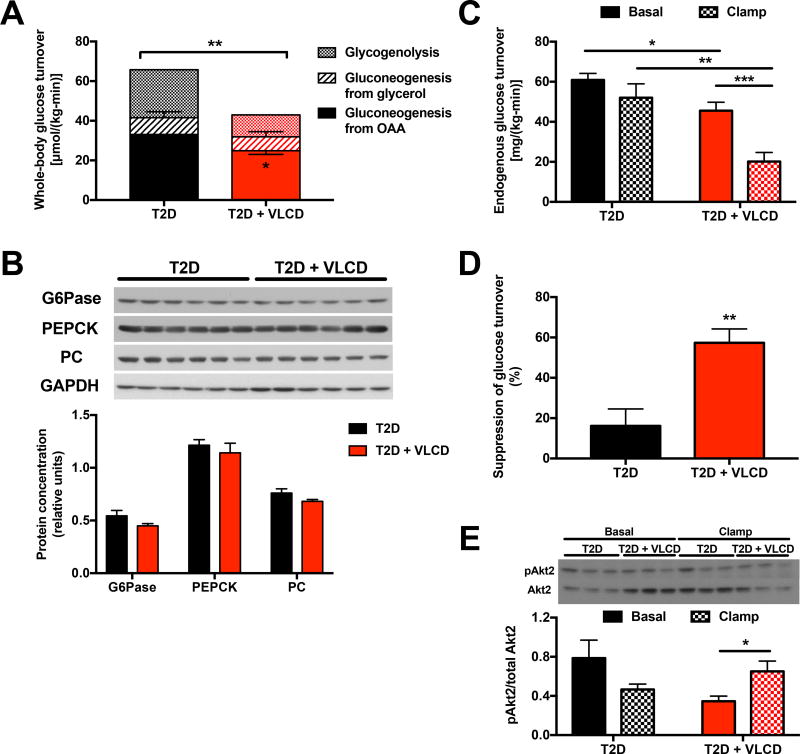
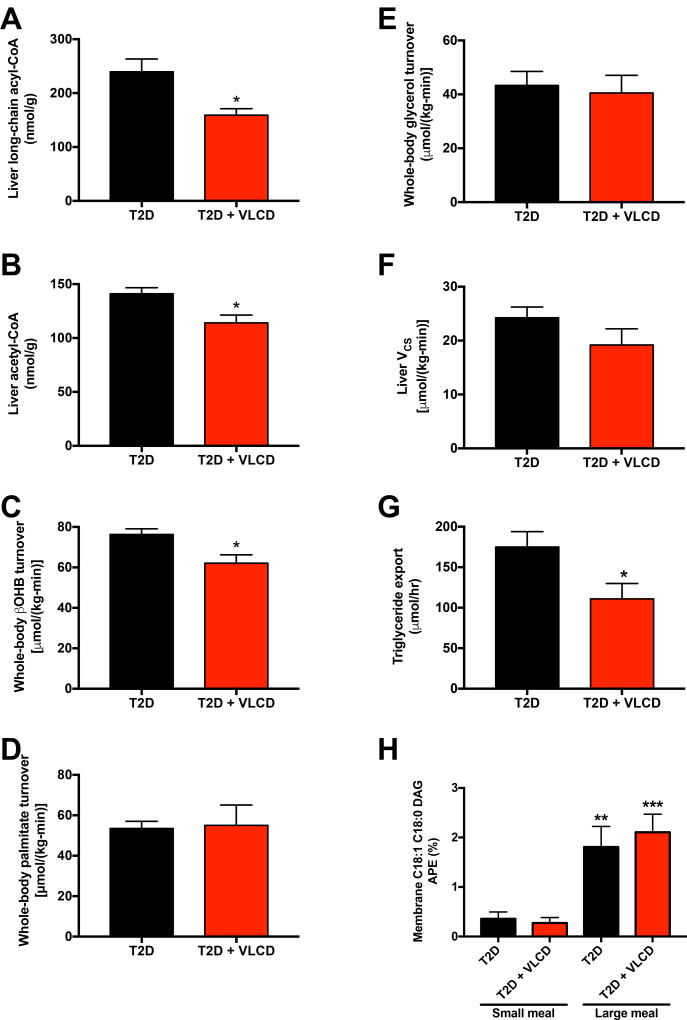
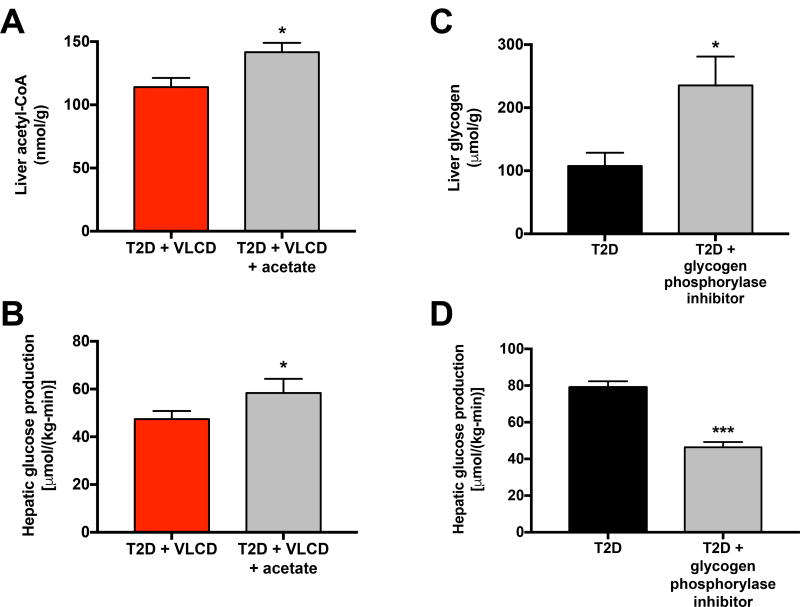
Caloric restriction rapidly reverses type 2 diabetes (T2D), but the mechanism(s) of this reversal are poorly understood. Here we show that 3 days of a very-low-calorie diet (VLCD, one-quarter their typical intake) lowered plasma glucose and insulin concentrations in a rat model of T2D without altering body weight. The lower plasma glucose was associated with a 30% reduction in hepatic glucose production resulting from suppression of both gluconeogenesis from pyruvate carboxylase (VPC), explained by a reduction in hepatic acetyl-CoA content, and net hepatic glycogenolysis. In addition, VLCD resulted in reductions in hepatic triglyceride and diacylglycerol content and PKCɛ translocation, associated with improved hepatic insulin sensitivity. Taken together, these data show that there are pleotropic mechanisms by which VLCD reverses hyperglycemia in a rat model of T2D, including reduced DAG-PKCɛ-induced hepatic insulin resistance, reduced hepatic glycogenolysis, and reduced hepatic acetyl-CoA content, PC flux, and gluconeogenesis.
Keywords: T2D; acetyl-CoA; caloric restriction; gluconeogenesis; glycogenolysis; type 2 diabetes; very low calorie diet; very-low-calorie diet.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare that no conflicts of interest exist.
Figures
Comment in
-
Diabetes: Very-low-calorie diet reverses T2DM in rats.Nat Rev Endocrinol. 2018 Jan;14(1):2. doi: 10.1038/nrendo.2017.159. Epub 2017 Nov 24. Nat Rev Endocrinol. 2018. PMID: 29170538 No abstract available.
References
-
- Bligh EG, Dyer WJ. A rapid method of total lipid extraction and purification. Canadian journal of biochemistry and physiology. 1959;37:911–917. - PubMed
-
- Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K, Schoelles K. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724–1737. - PubMed
-
- Buchwald H, Estok R, Fahrbach K, Banel D, Jensen MD, Pories WJ, Bantle JP, Sledge I. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. The American journal of medicine. 2009;122:248–256. e245. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
