

Contemporary Epidemiology of Heart Failure in Fee-For-Service Medicare Beneficiaries Across Healthcare Settings
- PMID: 29129828
- PMCID: PMC6057614
- DOI: 10.1161/CIRCHEARTFAILURE.117.004402
Contemporary Epidemiology of Heart Failure in Fee-For-Service Medicare Beneficiaries Across Healthcare Settings
Abstract
Background: To assess the current landscape of the heart failure (HF) epidemic and provide targets for future health policy interventions in Medicare, a contemporary appraisal of its epidemiology across inpatient and outpatient care settings is needed.
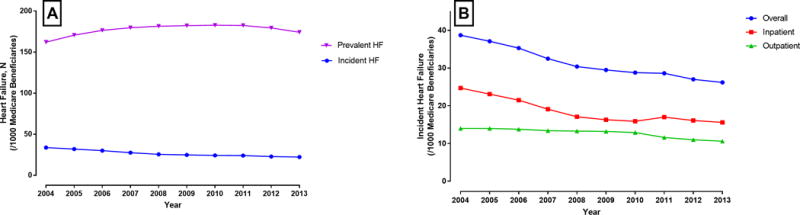
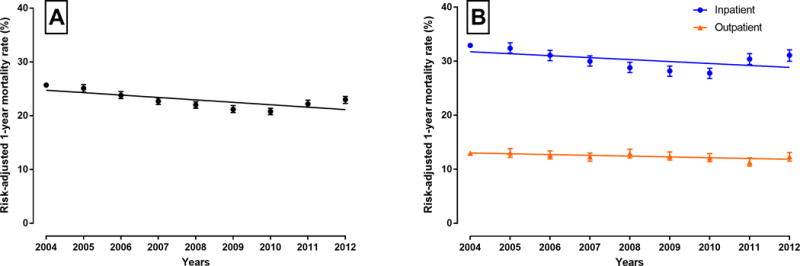
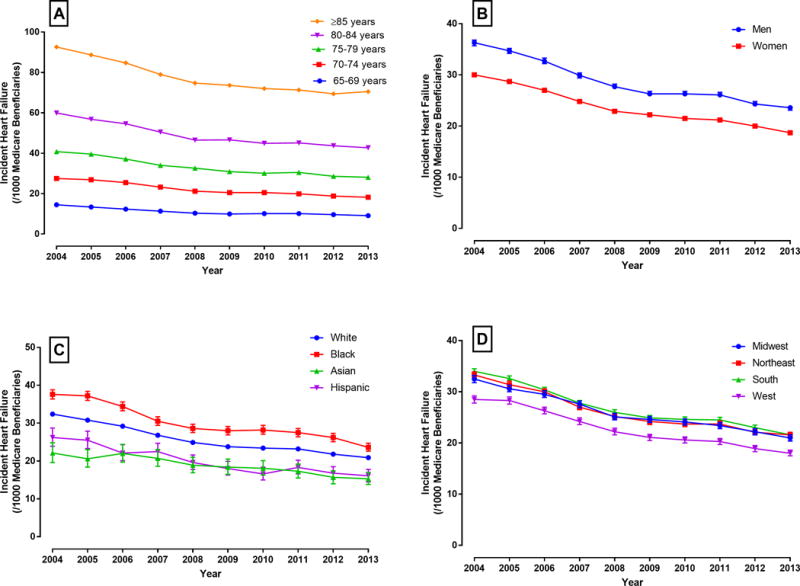
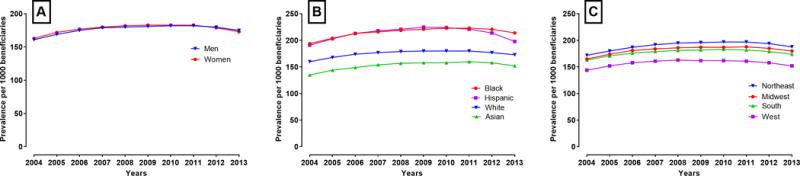
Methods and results: In a national 5% sample of Medicare beneficiaries from 2002 to 2013, we identified a cohort of 2 331 939 unique fee-for-service Medicare beneficiaries ≥65-years-old followed for all inpatient and outpatient encounters over a 10-year period (2004-2013). Preexisting HF was defined by any HF encounter during the first year, and incident HF with either 1 inpatient or 2 outpatient HF encounters. Mean age of the cohort was 72 years; 57% were women, and 86% and 8% were white and black, respectively. Within this cohort, 518 223 patients had preexisting HF, and 349 826 had a new diagnosis of HF during the study period. During 2004 to 2013, the rates of incident HF declined 32%, from 38.7 per 1000 (2004) to 26.2 per 1000 beneficiaries (2013). In contrast, prevalent (preexisting + incident) HF increased during our study period from 162 per 1000 (2004) to 172 per 1000 beneficiaries (2013) (Ptrend <0.001 for both). Finally, the overall 1-year mortality among patients with incident HF is high (24.7%) with a 0.4% absolute decline annually during the study period, with a more pronounced decrease among those diagnosed in an inpatient versus outpatient setting (Pinteraction <0.001) CONCLUSIONS: In recent years, there have been substantial changes in the epidemiology of HF in Medicare beneficiaries, with a decline in incident HF and a decrease in 1-year HF mortality, whereas the overall burden of HF continues to increase.
Keywords: Medicare; health policy; heart failure; hospitalization; incidence.
© 2017 American Heart Association, Inc.
Conflict of interest statement
Figures
References
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American Heart Association Statistics C and Stroke Statistics S Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation. 2017;135:e146–e603. - PMC - PubMed
-
- Roger VL, Weston SA, Redfield MM, Hellermann-Homan JP, Killian J, Yawn BP, Jacobsen SJ. Trends in heart failure incidence and survival in a community-based population. JAMA. 2004;292:344–50. - PubMed
-
- Croft JB, Giles WH, Pollard RA, Casper ML, Anda RF, Livengood JR. National trends in the initial hospitalization for heart failure. J Am Geriatr Soc. 1997;45:270–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
