

The Electrophysiological Substrate of Early Repolarization Syndrome: Noninvasive Mapping in Patients
- PMID: 29130071
- PMCID: PMC5675574
- DOI: 10.1016/j.jacep.2016.12.017
The Electrophysiological Substrate of Early Repolarization Syndrome: Noninvasive Mapping in Patients
Abstract
Background: The early repolarization (ER) pattern is a common ECG finding. Recent studies established a definitive clinical association between ER and fatal ventricular arrhythmias. However, the arrhythmogenic substrate of ER in the intact human heart has not been characterized.
Objectives: To map the epicardial electrophysiological (EP) substrate in ER syndrome patients using noninvasive Electrocardiographic Imaging (ECGI), and to characterize substrate properties that support arrhythmogenicity.
Methods: Twenty-nine ER syndrome patients were enrolled, 17 of which had a malignant syndrome. Characteristics of the abnormal EP substrate were analyzed using data recorded during sinus rhythm. The EP mapping data were analyzed for electrogram morphology, conduction and repolarization. Seven normal subjects provided control data.
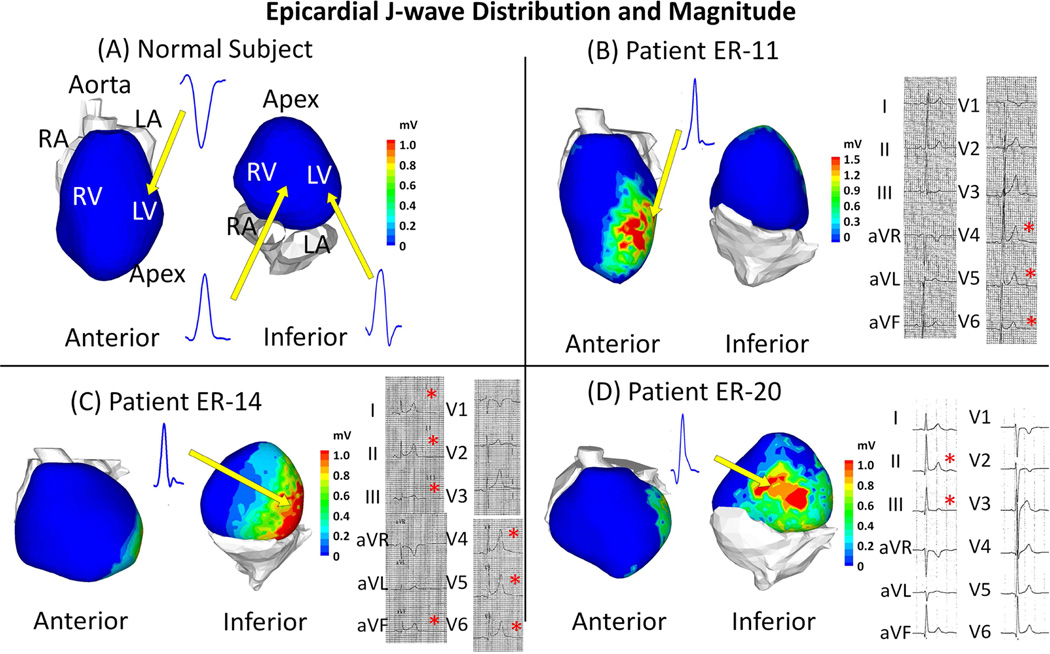
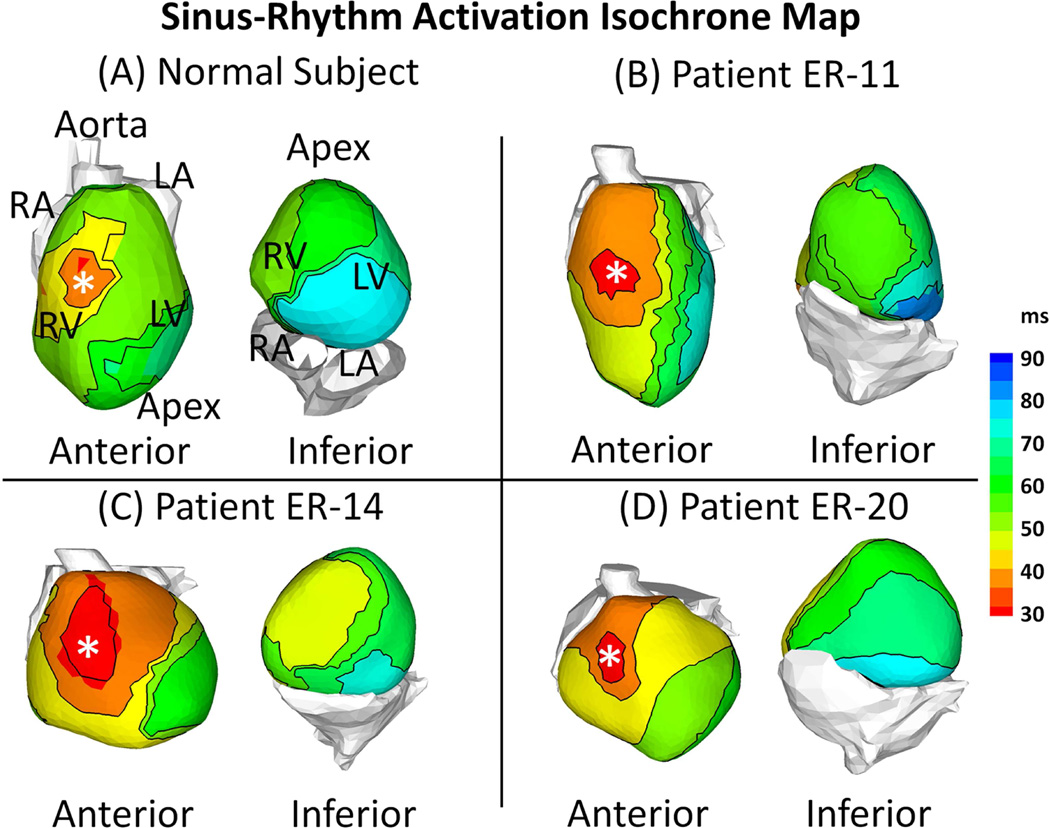
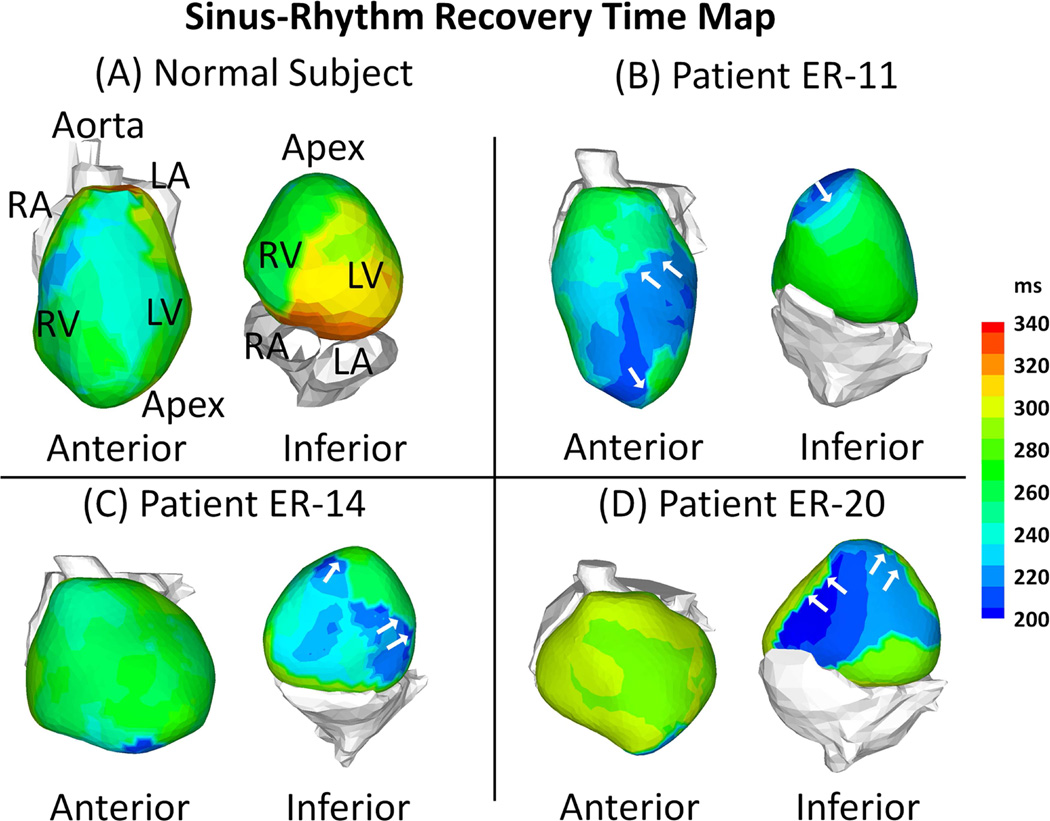
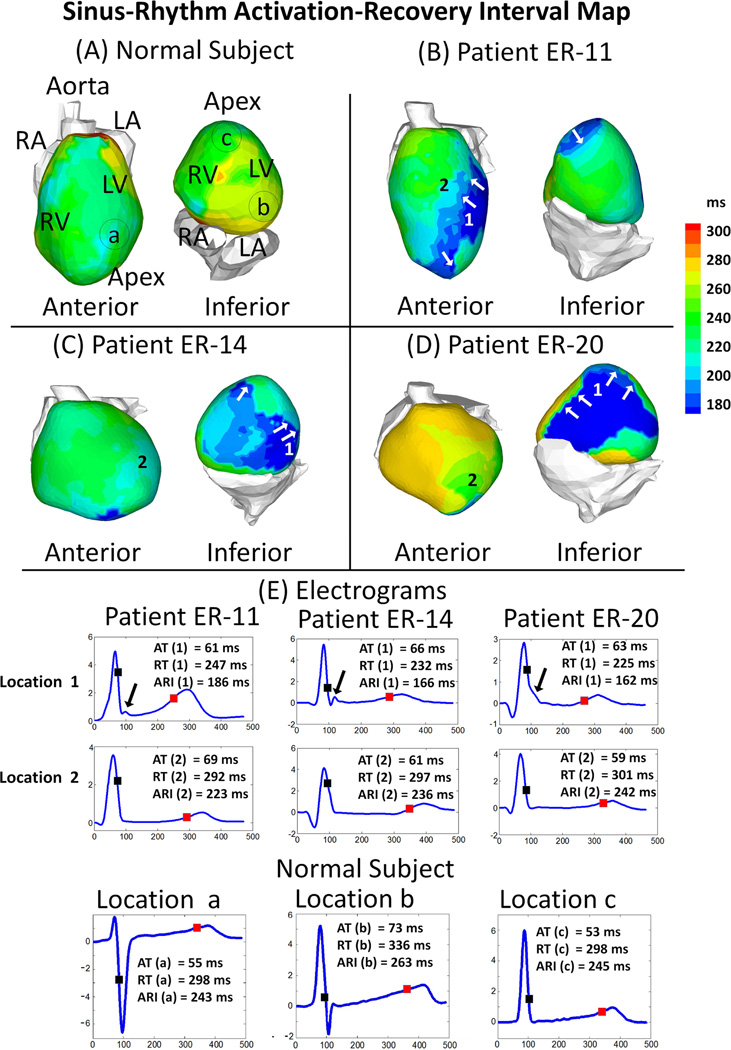
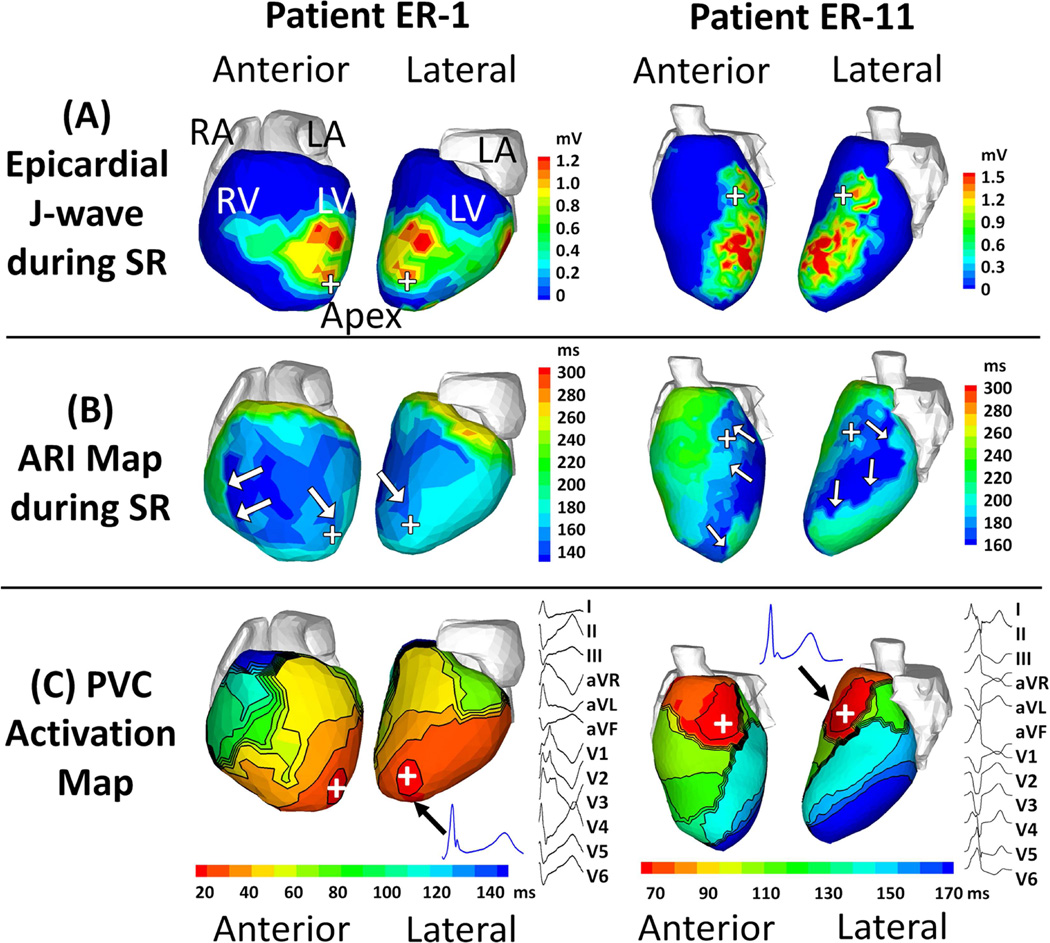
Results: The abnormal EP substrate in ER syndrome patients has the following properties: (1) Abnormal epicardial electrograms characterized by presence of J-waves in localized regions; (2) Absence of conduction abnormalities, including delayed activation, conduction block, or fractionated electrograms; (3) Marked abbreviation of ventricular repolarization in areas with J-waves. The action potential duration (APD) was significantly shorter than normal (196±19 vs. 235±21 ms, p<0.05). Shortening of APD occurred heterogeneously, leading to steep repolarization gradients compared to normal control (45±17 vs.7±5 ms/cm, p<0.05). Premature ventricular contractions (PVCs) were recorded in 2 patients. The PVC sites of origin were closely related to the abnormal EP substrate with J-waves and steep repolarization gradients.
Conclusions: Early Repolarization is associated with steep repolarization gradients caused by localized shortening of APD. Results suggest association of PVC initiation sites with areas of repolarization abnormalities. Conduction abnormalities were not observed.
Keywords: early repolarization; idiopathic ventricular fibrillation; mapping; sudden cardiac death.
Figures
References
-
- Haissaguerre M, Derval N, Sacher F, et al. Sudden cardiac arrest associated with early repolarization. N Engl J Med. 2008;358:2016–2023. - PubMed
-
- Tikkanen JT, Anttonen O, Junttila J, et al. Long-term outcome associated with early repolarization on electrocardiography. N Engl J Med. 2009;361:2529–2537. - PubMed
-
- Kambara H, Phillips J. Long-term evaluation of early repolarization syndrome (normal variant rst segment elevation) Am J Cardiol. 1976;38:157–161. - PubMed
-
- Gussak I, Antzelevitch C. Early repolarization syndrome: Clinical characteristics and possible cellular and ionic mechanisms. J Electrocardiol. 2000;33:299–309. - PubMed
-
- Boineau JP. The early repolarization variant--normal or a marker of heart disease in certain subjects. J Electrocardiol. 2007;40:3, e11–e16. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical