

Shifting Patterns in Cesarean Delivery Scheduling and Timing in Oregon before and after a Statewide Hard Stop Policy
- PMID: 29131330
- PMCID: PMC6056593
- DOI: 10.1111/1475-6773.12797
Shifting Patterns in Cesarean Delivery Scheduling and Timing in Oregon before and after a Statewide Hard Stop Policy
Abstract
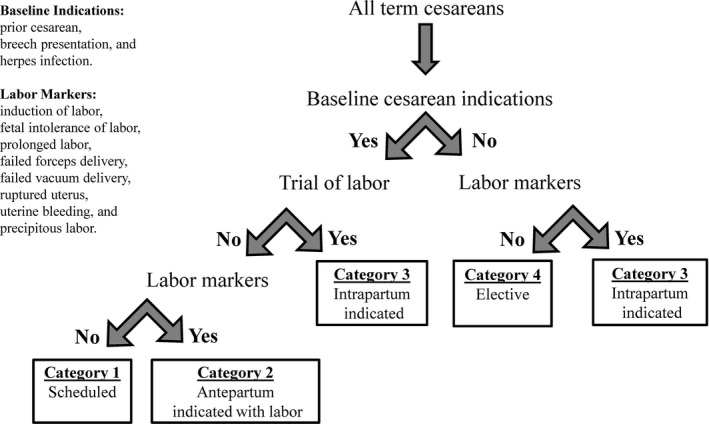
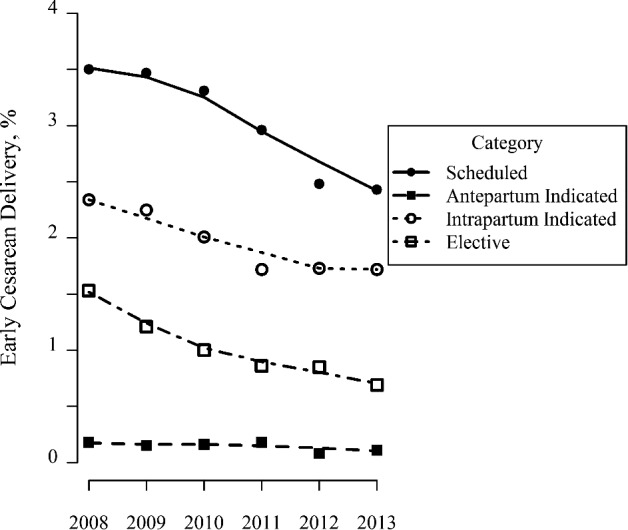
Objectives: To assess the use and timing of scheduled cesareans and other categories of cesarean delivery and the prevalence of neonatal morbidity among cesareans in Oregon before and after the implementation of Oregon's statewide policy limiting elective early deliveries.
Data sources: Oregon vital statistics records, 2008-2013.
Study design: Retrospective cohort study, with multivariable logistic regression, regression controlling for time trends, and interrupted time series analyses, to compare the odds of different categories of cesarean delivery and the odds of neonatal morbidity pre- and postpolicy.
Data collection/extraction methods: We analyzed vital statistics data on all term births in Oregon (2008-2013), excluding births in 2011.
Principal findings: The odds of early-term scheduled cesareans decreased postpolicy (adjusted odds ratio [aOR], 0.70; 95 percent confidence interval [CI], 0.66-0.74). In the postpolicy period, there were mixed findings regarding assisted neonatal ventilation and neonatal intensive care unit admission, with regression models indicating higher postpolicy odds in some categories, but lower postpolicy odds after controlling for time trends.
Conclusions: Oregon's hard stop policy limiting elective early-term cesarean delivery was associated with lower odds of cesarean delivery in the category of women who were targeted by the policy; more research is needed on impact of such policies on neonatal outcomes.
Keywords: Health policy/politics/law/regulation; maternal and perinatal care and outcomes; obstetrics/gynecology.
© Health Research and Educational Trust.
Figures
References
-
- ACOG (American College of Obstetricians, Gynecologists) . 2013. “ACOG Committee Opinion no. 560: Medically Indicated Late‐Preterm and Early‐Term Deliveries.” Obstetrics and Gynecology 121 (4): 908–10. - PubMed
-
- ACOG (American College of Obstetricians & Gynecologists) , and SMFM (Society for Maternal‐Fetal Medicine) . 2014. “Obstetric Care Consensus No. 1: Safe Prevention of the Primary Cesarean Delivery.” Obstetrics and Gynecology 123 (3): 693–711. - PubMed
-
- Basso, O. 2016. “Implications of Using a Fetuses‐at‐Risk Approach When Fetuses Are Not at Risk.” Paediatric and Perinatal Epidemiology 30 (1): 3–10. - PubMed
-
- Caughey, A. B. , and Snowden J. M.. 2016. “Measuring Perinatal Complications: Different Approaches Depending on Who Is at Risk.” Paediatric and Perinatal Epidemiology 30 (1): 23–4. - PubMed
-
- Cheng, Y. W. , Nicholson J. M., Nakagawa S., Bruckner T. A., Washington A. E., and Caughey A. B.. 2008. “Perinatal Outcomes in Low‐Risk Term Pregnancies: Do They Differ By Week of Gestation?” American Journal of Obstetrics and Gynecology 199 (4): 370.e1–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
