

Catheter-Directed Thrombolysis Versus Standard Anticoagulation for Acute Lower Extremity Deep Vein Thrombosis: A Meta-Analysis of Clinical Trials
- PMID: 29132220
- PMCID: PMC6714738
- DOI: 10.1177/1076029617739703
Catheter-Directed Thrombolysis Versus Standard Anticoagulation for Acute Lower Extremity Deep Vein Thrombosis: A Meta-Analysis of Clinical Trials
Abstract
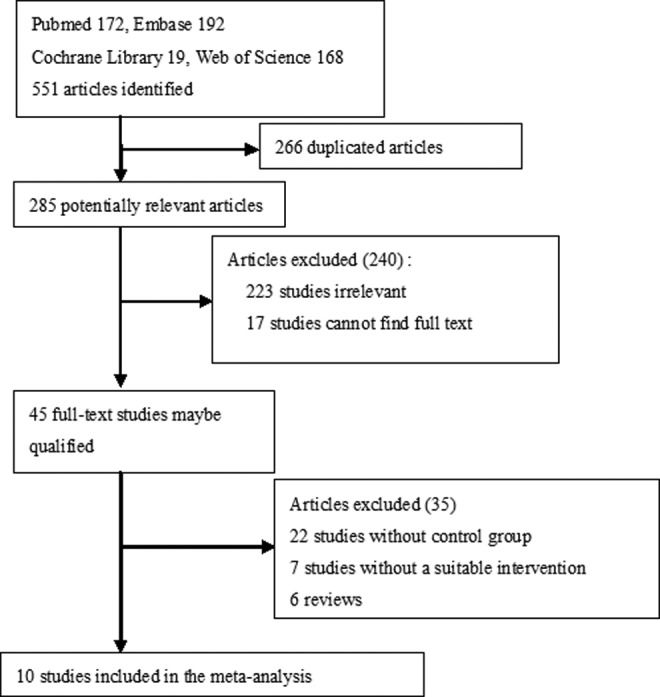
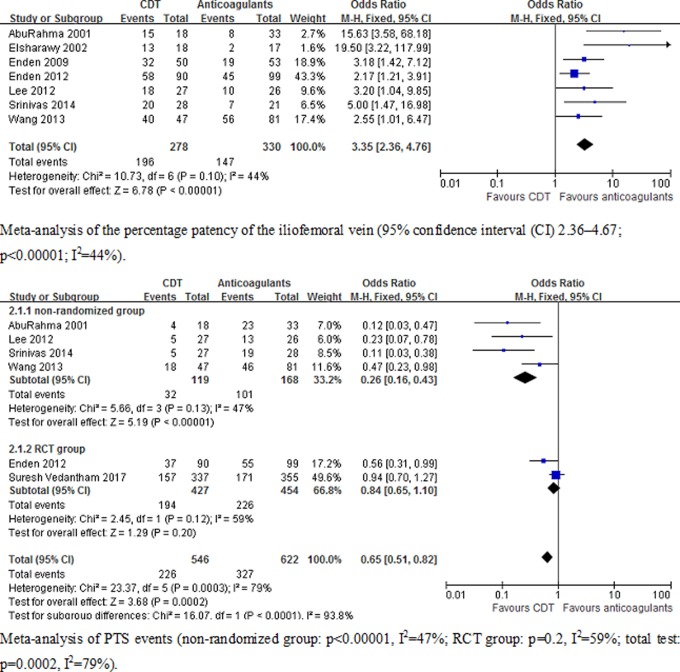
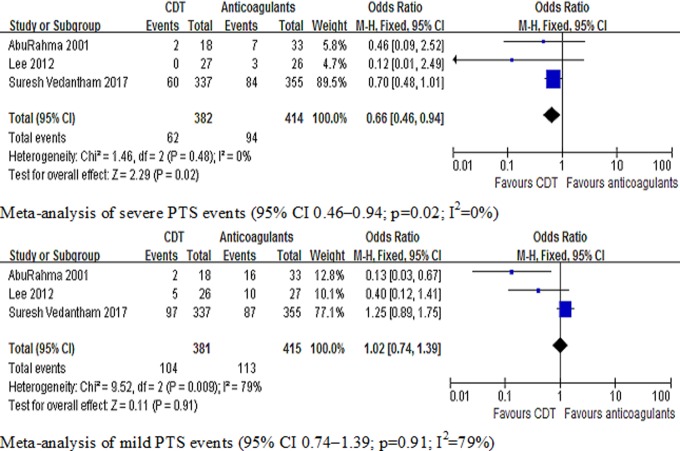
Standard anticoagulant treatment alone for acute lower extremity deep vein thrombosis (DVT) is ineffective in eliminating thrombus from the deep venous system, with many patients developing postthrombotic syndrome (PTS). Because catheter-directed thrombolysis (CDT) can dissolve the clot, reducing the development of PTS in iliofemoral or femoropopliteal DVT. This meta-analysis compares CDT plus anticoagulation versus standard anticoagulation for acute iliofemoral or femoropopliteal DVT. Ten trials were included in the meta-analysis. Compared with anticoagulant alone, CDT was shown to significantly increase the percentage patency of the iliofemoral vein ( P < .00001; I2 = 44%) and reduce the risk of PTS ( P = .0002; I2 = 79%). In subgroup analysis of randomized controlled trials, CDT was not shown to prevent PTS ( P = .2; I2 = 59%). A reduced PTS risk was shown, however, in nonrandomized trials ( P < .00001; I2 = 47%). Meta-analysis showed that CDT can reduce severe PTS risk ( P = .002; I2 = 0%). However, CDT was not indicated to prevent mild PTS ( P = .91; I2 = 79%). A significant increase in bleeding events ( P < .00001; I2 = 33%) and pulmonary embolism (PE) ( P < .00001; I2 = 14%) were also demonstrated. However, for the CDT group, the duration of stay in the hospital was significantly prolonged compared to the anticoagulant group ( P < .00001; I2 = 0%). There was no significant difference in death ( P = .09; I2 = 0%) or recurrent venous thromboembolism events ( P = .52; I2 = 58%). This meta-analysis showed that CDT may improve patency of the iliofemoral vein or severe PTS compared with anticoagulation therapy alone, but measuring PTS risk remains controversial. However, CDT could increase the risk of bleeding events, PE events, and duration of hospital stay.
Keywords: anticoagulation; catheter-directed thrombolysis; deep vein thrombosis (DVT).
Conflict of interest statement
Figures


Similar articles
-
Thrombolytic strategies versus standard anticoagulation for acute deep vein thrombosis of the lower limb.Cochrane Database Syst Rev. 2021 Jan 19;1(1):CD002783. doi: 10.1002/14651858.CD002783.pub5. Cochrane Database Syst Rev. 2021. PMID: 33464575 Free PMC article.
-
Catheter-directed thrombolysis plus anticoagulation versus anticoagulation alone in the treatment of proximal deep vein thrombosis - a meta-analysis.Vasa. 2015 May;44(3):195-202. doi: 10.1024/0301-1526/a000430. Vasa. 2015. PMID: 26098323 Review.
-
Pharmacomechanical Thrombectomy Versus Catheter-Directed Thrombolysis for Iliofemoral Deep Vein Thrombosis: A Meta-Analysis of Clinical Trials.Clin Appl Thromb Hemost. 2019 Jan-Dec;25:1076029618821190. doi: 10.1177/1076029618821190. Clin Appl Thromb Hemost. 2019. PMID: 30808224 Free PMC article.
-
Evaluation of thrombolysis using tissue plasminogen activator in lower extremity deep venous thrombosis with concomitant femoral-popliteal venous segment involvement.J Vasc Surg Venous Lymphat Disord. 2017 Sep;5(5):613-620. doi: 10.1016/j.jvsv.2017.04.018. Epub 2017 Jun 21. J Vasc Surg Venous Lymphat Disord. 2017. PMID: 28818211
-
Long-term outcome after additional catheter-directed thrombolysis versus standard treatment for acute iliofemoral deep vein thrombosis (the CaVenT study): a randomised controlled trial.Lancet. 2012 Jan 7;379(9810):31-8. doi: 10.1016/S0140-6736(11)61753-4. Epub 2011 Dec 13. Lancet. 2012. PMID: 22172244 Clinical Trial.
Cited by
-
Comparison of Treatment Result Between Anticoagulation Alone and Catheter-Directed Thrombolysis Plus Anticoagulation in Acute Lower Extremity Deep Vein Thrombosis.Vasc Specialist Int. 2019 Mar;35(1):28-33. doi: 10.5758/vsi.2019.35.1.28. Vasc Specialist Int. 2019. PMID: 30993105 Free PMC article.
-
Does Catheter-Directed Thrombolysis Prevent Postthrombotic Syndrome?Vasc Specialist Int. 2018 Jun;34(2):26-30. doi: 10.5758/vsi.2018.34.2.26. Epub 2018 Jun 30. Vasc Specialist Int. 2018. PMID: 29984214 Free PMC article.
-
Single-Session Percutaneous Mechanical Thrombectomy Using the Aspirex®S Device Plus Stenting for Acute Iliofemoral Deep Vein Thrombosis: Safety, Efficacy, and Mid-Term Outcomes.Diagnostics (Basel). 2020 Jul 30;10(8):544. doi: 10.3390/diagnostics10080544. Diagnostics (Basel). 2020. PMID: 32751767 Free PMC article.
-
Endovascular Therapy for Venous Thromboembolic Diseases.Acta Cardiol Sin. 2021 Nov;37(6):566-573. doi: 10.6515/ACS.202111_37(6).20210505B. Acta Cardiol Sin. 2021. PMID: 34812229 Free PMC article. Review.
-
Single- versus multiple-stage catheter-directed thrombolysis for acute iliofemoral deep venous thrombosis does not have an impact on iliac vein stent length or patency rates.J Vasc Surg Venous Lymphat Disord. 2019 Nov;7(6):781-788. doi: 10.1016/j.jvsv.2019.05.010. Epub 2019 Sep 5. J Vasc Surg Venous Lymphat Disord. 2019. PMID: 31495769 Free PMC article.
References
-
- Lee CH, Cheng CL, Lin LJ, Tsai LM, Yang YH. Epidemiology and predictors of short-term mortality in symptomatic venous thromboembolism. Circ J. 2011;75(8):1998–2004. - PubMed
-
- Kahn SR. The post-thrombotic syndrome: progress and pitfalls. Br J Haematol. 2006;134(4):357–365. - PubMed
-
- Kahn SR, Elman EA, Bornais C, Blostein M, Wells PS. Post-thrombotic syndrome, functional disability and quality of life after upper extremity deep venous thrombosis in adults. Thromb Hemost. 2005;93(3):499–502. - PubMed
-
- Amin VB, Lookstein RA. Catheter-directed interventions for acute iliocaval deep vein thrombosis. Tech Vasc Interv Radiol. 2014;17(2):96–102. - PubMed
-
- Guanella R, Ducruet T, Johri M, et al. Economic burden and cost determinants of deep vein thrombosis during 2 years following diagnosis: a prospective evaluation. J Thromb Haemost. 2011;9(12):2397–2405. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
