

Level, causes, and risk factors of stillbirth: a population-based case control study from Chandigarh, India
- PMID: 29132325
- PMCID: PMC5684767
- DOI: 10.1186/s12884-017-1557-4
Level, causes, and risk factors of stillbirth: a population-based case control study from Chandigarh, India
Abstract
Background: Globally, India ranks first in the absolute number of stillbirths. Hence, the level, causes, and risk factors of stillbirths were estimated to facilitate designing of prevention strategy.
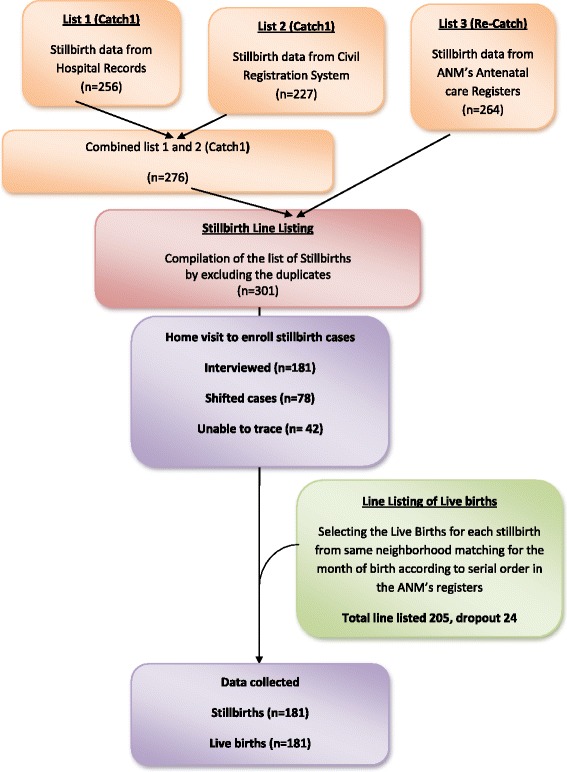
Methods: Capture and recapture method was used to identify 301 stillbirths from 1st July 2013 to 31st August 2014 in Chandigarh Union Territory of India. Verbal autopsies (n = 181) were done at household level to identify causes of stillbirths. Risk factors were determined using case-control approach. Women who had a stillbirth in the past 3 months were enrolled as cases (n = 181) and those who had live-birth in same neighbourhood were included as controls (n = 181). Statistical differences in the distribution of characteristics of cases and controls were tested by t test and chi square test respectively for quantitative and categorical variables. In logistic regression models adjusted odds ratios (aOR) and 95% confidence intervals (CIs) were estimated for various risk factors.
Results: Stillbirth rate was estimated to be 16/1000 birth. Antepartum causes were more common (68%) than intrapartum causes (32%). Among maternal conditions, hypertension (18.2%) and chorio-amnionitis (13.8%), and among foetal conditions, growth restriction (19.9%) and congenital anomalies (18.8%) were the leading causes. In about half of the stillbirths foetal (48%) and maternal (44.7%) causes were unidentifiable. Risk factors of stillbirths were: higher maternal age (aOR 1.1, 95%CI 1.0-1.2), vaginal delivery (aOR 8.1, 95%CI 2.6-26), induced labour (aOR 2.6, 95%CI 1.5-4.5), green or light brown liquor (aOR 2.0, 95%CI 1.1-3.8), preterm delivery (aOR 6.4, 95%CI 3.7-11) and smaller household size (aOR 1.2, 95% CI 1.1-1.3).
Conclusions: Stillbirth rate was high in Chandigarh Union Territory of India. Major causes and risk factors amenable to interventions were infections, hypertension, congenital malformations, foetal growth restriction, pre-maturity and household size. Therefore, better maternity ante-natal and intra-natal care is required to achieve a single digit stillbirth rate.
Keywords: Capture and recapture; Case control; Fetal death; Incidence; India; Pregnancy outcome; Risk factors; Stillbirth.
Conflict of interest statement
Author’s information
Designations:
1Junior Resident of Community Medicine, 2,Additional Professor of Health Promotion, 3Addtional Professor of Community Medicine, 4Professor of Community Medicine and Head of Department.
Institutional Affiliations: Department of Community Medicine & School of Public Health, Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, India.
Ethics approval and consent to participate
Ethical approval was obtained from the institute ethical committee to conduct this study (Reference NK/988/MD/13645). Prior written informed consent was obtained from every study participants.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
