

Tubeless versus standard percutaneous nephrolithotomy: an update meta-analysis
- PMID: 29132344
- PMCID: PMC5683212
- DOI: 10.1186/s12894-017-0295-2
Tubeless versus standard percutaneous nephrolithotomy: an update meta-analysis
Abstract
Background: To update a previously published systematic review and meta-analysis on the efficacy and safety of tubeless percutaneous nephrolithotomy (PCNL).
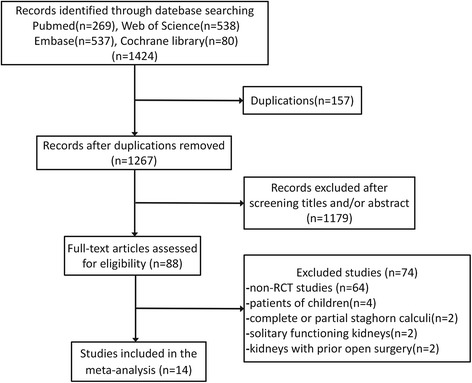
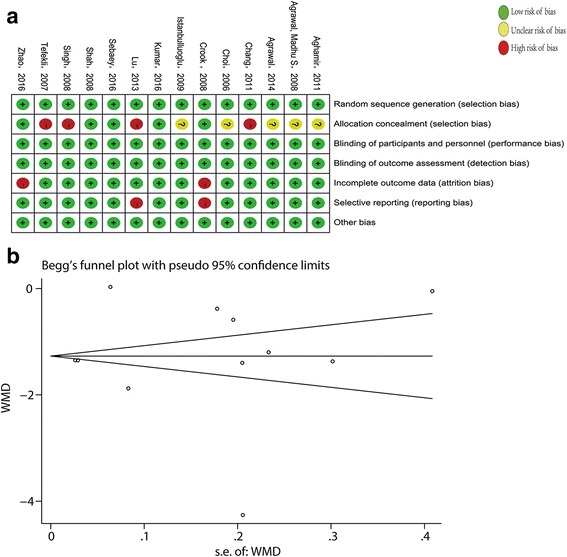
Methods: A systematic literature search of EMBASE, PubMed, Web of Science, and the Cochrane Library was performed to confirm relevant studies. The scientific literature was screened in accordance with the predetermined inclusion and exclusion criteria. After quality assessment and data extraction from the eligible studies, a meta-analysis was conducted using Stata SE 12.0.
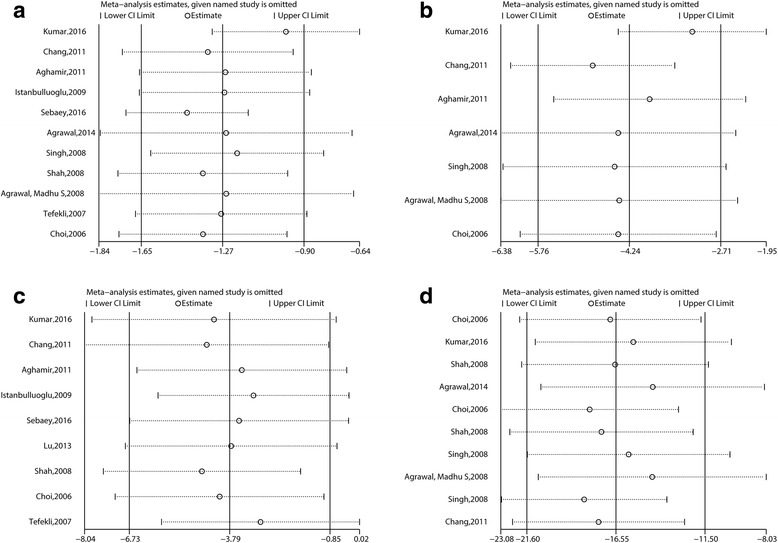
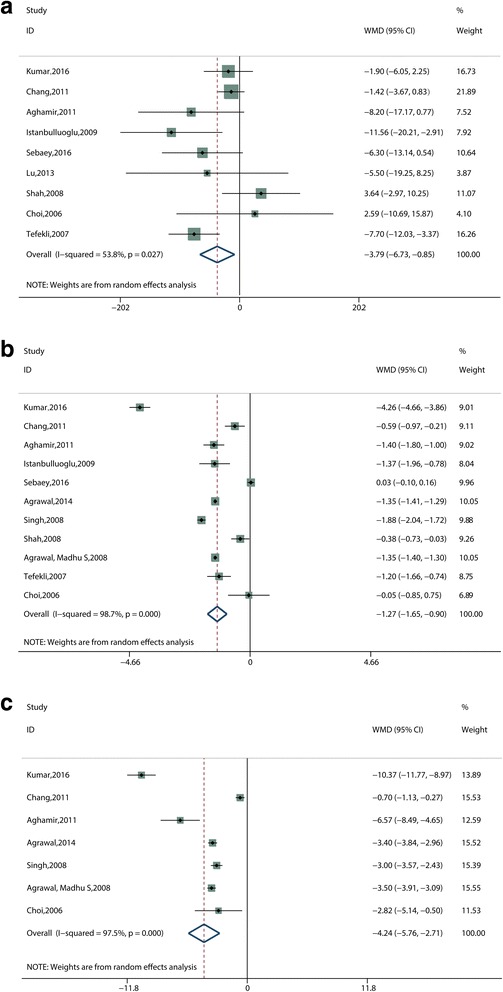
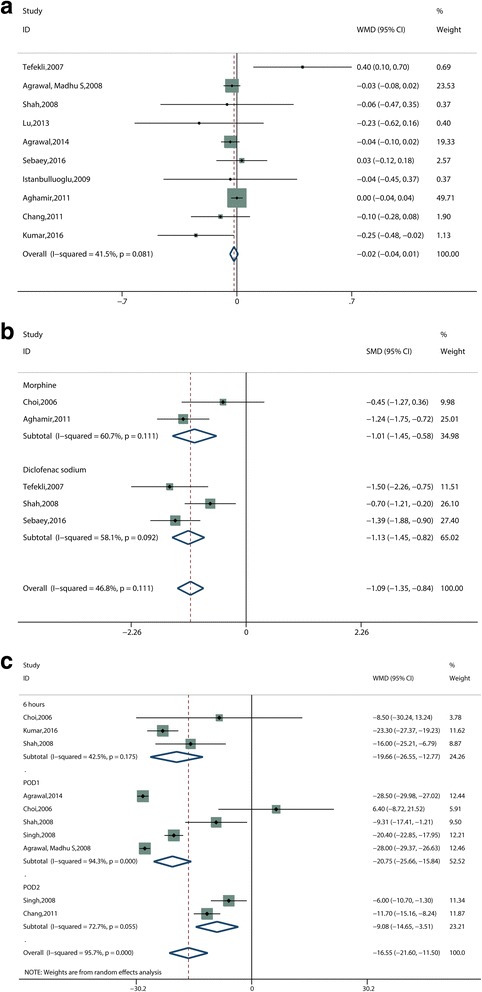
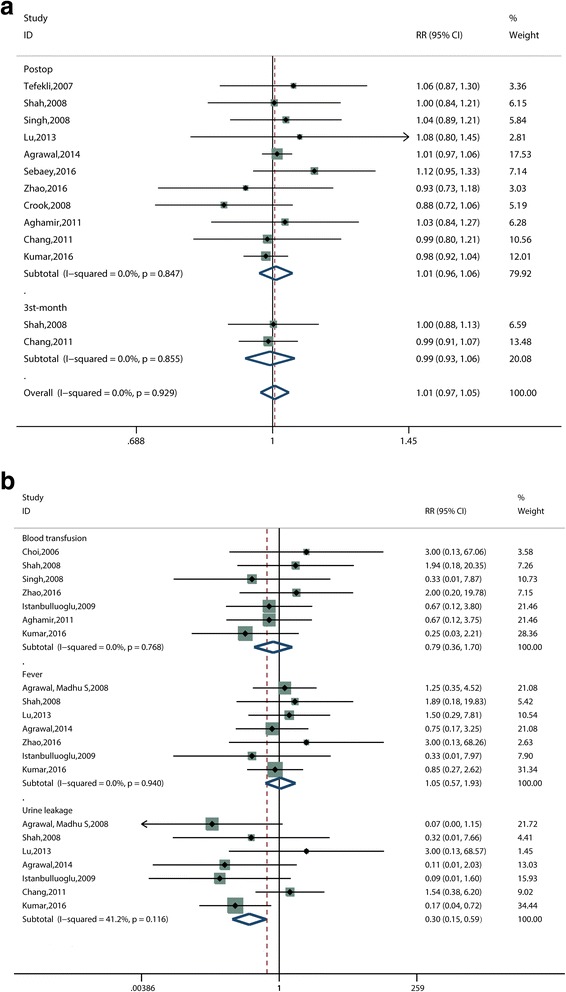
Results: Fourteen randomized controlled trials (RCTs) involving 1148 patients were included. Combined results demonstrated that tubeless PCNL was significantly associated with shorter operative time (weighted mean difference [WMD], -3.79 min; 95% confidence interval [CI], -6.73 to -0.85; P = 0.012; I2 = 53.8%), shorter hospital stay (WMD, -1.27 days; 95% CI, -1.65 to -0.90; P < 0.001; I2 = 98.7%), faster time to return to normal activity (WMD, -4.24 days; 95% CI, -5.76 to -2.71; P < 0.001; I2 = 97.5%), lower postoperative pain scores (WMD, -16.55 mm; 95% CI, -21.60 to -11.50; P < 0.001; I2 = 95.7%), less postoperative analgesia requirements (standard mean difference, -1.09 mg; 95% CI, -1.35 to -0.84; P < 0.001; I2 = 46.8%), and lower urine leakage (Relative risk [RR], 0.30; 95% CI 0.15 to 0.59; P = 0.001; I2 = 41.2%). There were no significant differences in postoperative hemoglobin reduction (WMD, -0.02 g/dL; 95% CI, -0.04 to 0.01; P = 0.172; I2 = 41.5%), stone-free rate (RR, 1.01; 95% CI, 0.97 to 1.05; P = 0.776; I2 = 0.0%), postoperative fever rate (RR, 1.05; 95% CI, 0.57 to 1.93; P = 0.867; I2 = 0.0%), or blood transfusion rate (RR, 0.79; 95% CI, 0.36 to 1.70; P = 0.538; I2 = 0.0%). The results of subgroup analysis were consistent with the overall findings. The sensitivity analysis indicated that most results remained constant when total tubeless or partial tubeless or mini-PCNL studies were excluded respectively.
Conclusions: Tubeless PCNL is an available and safe option in carefully evaluated and selected patients. It is significantly associated with the advantages of shorter hospital stay, shorter time to return to normal activity, lower postoperative pain scores, less analgesia requirement, and reduced urine leakage.
Keywords: Meta-analysis; PCNL; Percutaneous nephrolithotomy; Tubeless; Update.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Türk C, Neisius A, Petrik A, et al. Guidelines on urolithiasis. EAU. 2017. Available at: http://uroweb.org/guideline/urolithiasis/. Accessed 15 April 2017.
-
- Tirtayasa PMW, Yuri P, Birowo P, et al. Safety of tubeless or totally tubeless drainage and nephrostomy tube as a drainage following percutaneous nephrolithotomy: A comprehensive review. Asian J Surg. 2016;doi: 10.1016/j.asjsur.2016.03.003. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
