

Effect of frenotomy on breastfeeding variables in infants with ankyloglossia (tongue-tie): a prospective before and after cohort study
- PMID: 29132414
- PMCID: PMC5683371
- DOI: 10.1186/s12884-017-1561-8
Effect of frenotomy on breastfeeding variables in infants with ankyloglossia (tongue-tie): a prospective before and after cohort study
Abstract
Background: Controversy exists regarding ankyloglossia (tongue-tie) and its clinical impact on breastfeeding, including the benefits, or otherwise, of tongue-tie release (frenotomy). As exclusive breastfeeding rates in Ireland are already considerably low (46% on discharge home from the maternity unit following birth in 2014), it is imperative to protect and support breastfeeding, including identifying the associated effects that frenotomy might have on breastfeeding variables.
Objective: To determine the associated effects of frenotomy on breastfeeding variables in infants with ankyloglossia.
Methods: A prospective before and after cohort study was conducted. Following ethical approval, two self-reported questionnaires were administered to women whose infants were undergoing frenotomy at seven healthcare clinics in the Republic of Ireland. Data on breastfeeding variables prior to the frenotomy procedure and at 1-month post-frenotomy were collected and compared. Descriptive statistics (frequencies and proportions) were used to analyse, separately, the pre- and post-frenotomy data. Inferential statistics (z-test scores for differences between proportions (alpha <0.05) and mean differences (MD) with 95% confidence intervals (CI)) were used for pre- and post-frenotomy comparative analyses.
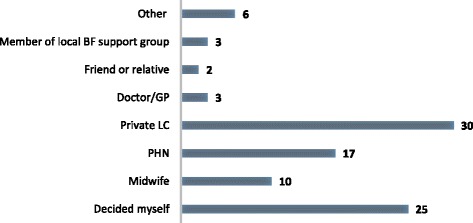
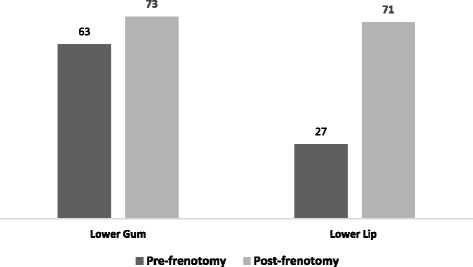
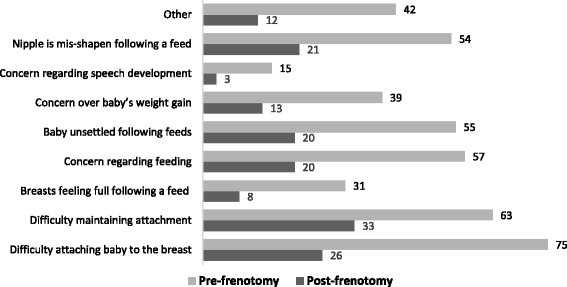
Results: Ninety-eight women returned the baseline questionnaire, and, of these, 89 returned the follow-up questionnaire. The most common reason for seeking a frenotomy was difficulty with latch (38%). Private lactation consultants were the main person recommending a frenotomy (31%). Rates of exclusive breastfeeding remained similar pre- and post-frenotomy (58% versus 58%), although rates of formula feeding increased two-fold at follow-up. Infants' ability to extend their tongues to the lower lip after frenotomy was significantly increased (p < 0.0001). Almost all participants (91%) reported an overall improvement in breastfeeding post-frenotomy. Pain on breastfeeding was significantly reduced post-frenotomy (MD 2.90, 95% CI 3.75 to 2.05) and overall LATCH scale scores were significantly increased (MD -0.50, 95% CI -0.67 to -0.33).
Conclusions: This study supports the hypothesis that frenotomy has a positive effect on breastfeeding variables in infants with ankyloglossia. These findings, however, are based on a relatively small number of participants from one country only where breastfeeding rates are low. Further, larger studies are required to substantiate these findings.
Keywords: Ankyloglossia; Breastfeeding; Frenotomy; Tongue-tie.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval to conduct the study was granted by the Research Ethics Committee of the School of Nursing & Midwifery, Trinity College Dublin. Written informed consent to participate in the study was obtained from all of the study participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
