

Uric Acid and the Risks of Kidney Failure and Death in Individuals With CKD
- PMID: 29132945
- PMCID: PMC5828916
- DOI: 10.1053/j.ajkd.2017.08.017
Uric Acid and the Risks of Kidney Failure and Death in Individuals With CKD
Abstract
Background: Serum uric acid concentrations increase in chronic kidney disease (CKD) and may lead to tubular injury, endothelial dysfunction, oxidative stress, and intrarenal inflammation. Whether uric acid concentrations are associated with kidney failure and death in CKD is unknown.
Study design: Prospective observational cohort study.
Settings & participants: 3,885 individuals with CKD stages 2 to 4 enrolled in the Chronic Renal Insufficiency Cohort (CRIC) between June 2003 and September 2008 and followed up through March 2013.
Predictor: Baseline uric acid concentrations.
Outcomes: Kidney failure (initiation of dialysis therapy or transplantation) and all-cause mortality.
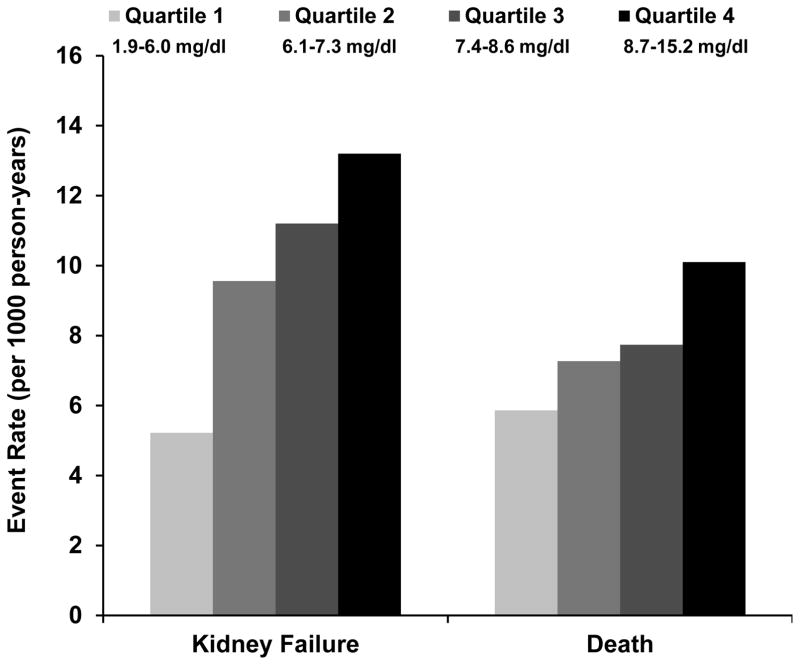
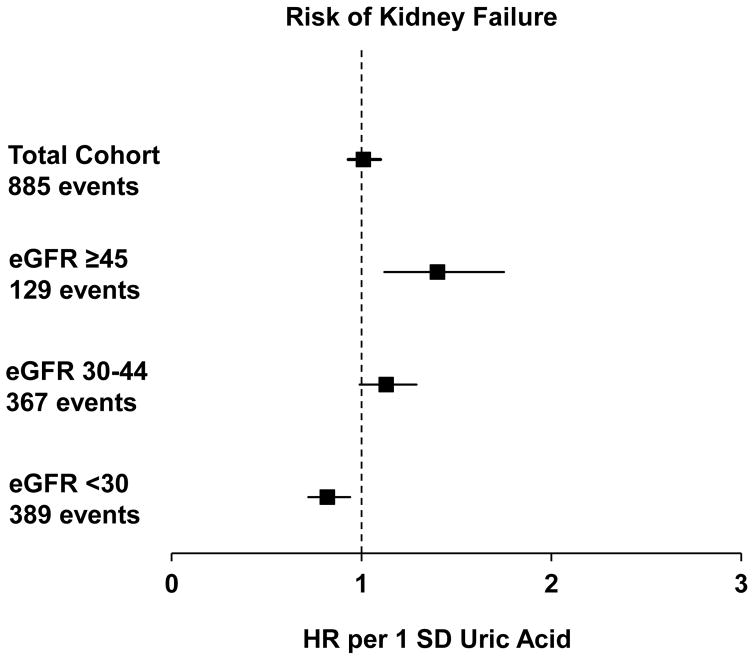
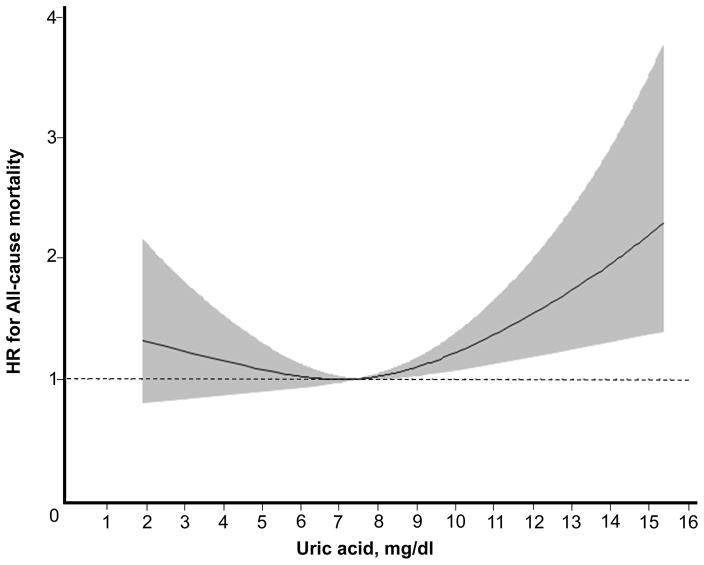
Results: During a median follow-up of 7.9 years, 885 participants progressed to kidney failure and 789 participants died. After adjustment for demographic, cardiovascular, and kidney-specific covariates, higher uric acid concentrations were independently associated with risk for kidney failure in participants with estimated glomerular filtration rates (eGFRs) ≥ 45mL/min/1.73m2 (adjusted HR per 1-standard deviation greater baseline uric acid, 1.40; 95% CI, 1.12-1.75), but not in those with eGFRs<30mL/min/1.73m2. There was a nominally higher HR in participants with eGFRs of 30 to 44mL/min/1.73m2 (adjusted HR, 1.13; 95% CI, 0.99-1.29), but this did not reach statistical significance. The relationship between uric acid concentration and all-cause mortality was J-shaped (P=0.007).
Limitations: Potential residual confounding through unavailable confounders; lack of follow-up measurements to adjust for changes in uric acid concentrations over time.
Conclusions: Uric acid concentration is an independent risk factor for kidney failure in earlier stages of CKD and has a J-shaped relationship with all-cause mortality in CKD. Adequately powered randomized placebo-controlled trials in CKD are needed to test whether urate lowering may prove to be an effective approach to prevent complications and progression of CKD.
Keywords: CKD progression; Chronic Renal Insufficiency Cohort (CRIC); Uric acid; chronic kidney disease (CKD); death; eGFR decline; end-stage renal disease (ESRD); hyperuricemia; kidney failure.
Copyright © 2017 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Masuo K, Kawaguchi H, Mikami H, Ogihara T, Tuck ML. Serum uric acid and plasma norepinephrine concentrations predict subsequent weight gain and blood pressure elevation. Hypertension. 2003;42(4):474–480. - PubMed
-
- Cirillo P, Sato W, Reungjui S, Heinig M, Gersch M, Sautin Y, et al. Uric acid, the metabolic syndrome, and renal disease. J Am Soc Nephrol. 2006;17(12 Suppl 3):S165–168. - PubMed
-
- Nakanishi N, Okamoto M, Yoshida H, Matsuo Y, Suzuki K, Tatara K. Serum uric acid and risk for development of hypertension and impaired fasting glucose or Type II diabetes in Japanese male office workers. Eur J Epidemiol. 2003;18(6):523–530. - PubMed
-
- Bos MJ, Koudstaal PJ, Hofman A, Witteman JC, Breteler MM. Uric acid is a risk factor for myocardial infarction and stroke: the Rotterdam study. Stroke. 2006;37(6):1503–1507. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
