

Characteristics and healthcare utilisation patterns of high-cost beneficiaries in the Netherlands: a cross-sectional claims database study
- PMID: 29133323
- PMCID: PMC5695517
- DOI: 10.1136/bmjopen-2017-017775
Characteristics and healthcare utilisation patterns of high-cost beneficiaries in the Netherlands: a cross-sectional claims database study
Abstract
Objective: To determine medical needs, demographic characteristics and healthcare utilisation patterns of the top 1% and top 2%-5% high-cost beneficiaries in the Netherlands.
Design: Cross-sectional study using 1 year claims data. We broke down high-cost beneficiaries by demographics, the most cost-incurring condition per beneficiary and expensive treatment use.
Setting: Dutch curative health system, a health system with universal coverage.
Participants: 4.5 million beneficiaries of one health insurer.
Measures: Annual total costs through hospital, intensive care unit use, expensive drugs, other pharmaceuticals, mental care and others; demographics; most cost-incurring and secondary conditions; inpatient stay; number of morbidities; costs per ICD10-chapter (International Statistical Classification of Diseases, 10th revision); and expensive treatment use (including dialysis, transplant surgery, expensive drugs, intensive care unit and diagnosis-related groups >€30 000).
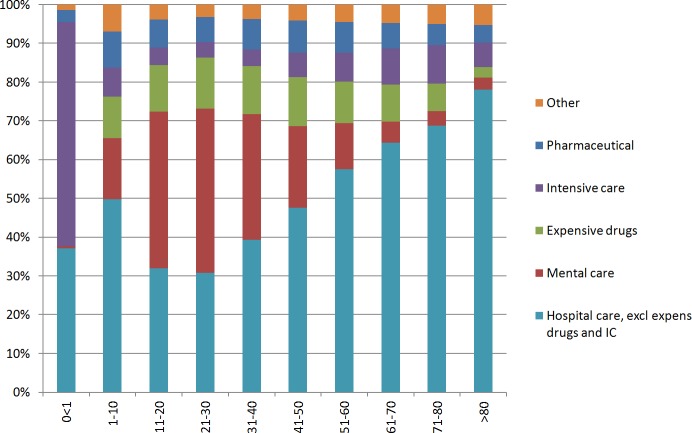
Results: The top 1% and top 2%-5% beneficiaries accounted for 23% and 26% of total expenditures, respectively. Among top 1% beneficiaries, hospital care represented 76% of spending, of which, respectively, 9.0% and 9.1% were spent on expensive drugs and ICU care. We found that 54% of top 1% beneficiaries were aged 65 years or younger and that average costs sharply decreased with higher age within the top 1% group. Expensive treatments contributed to high costs in one-third of top 1% beneficiaries and in less than 10% of top 2%-5% beneficiaries. The average number of conditions was 5.5 and 4.0 for top 1% and top 2%-5% beneficiaries, respectively. 53% of top 1% beneficiaries were treated for circulatory disorders but for only 22% of top 1% beneficiaries this was their most cost-incurring condition.
Conclusions: Expensive treatments, most cost-incurring condition and age proved to be informative variables for studying this heterogeneous population. Expensive treatments play a substantial role in high-costs beneficiaries. Interventions need to be aimed at beneficiaries of all ages; a sole focus on the elderly would leave many high-cost beneficiaries unaddressed. Tailored interventions are needed to meet the needs of high-cost beneficiaries and to avoid waste of scarce resources.
Keywords: health policy; high-cost patients; quality in health care.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
[Characteristics and healthcare utilization of patients with highest costs of care].Ned Tijdschr Geneeskd. 2017;161:D2220. Ned Tijdschr Geneeskd. 2017. PMID: 29219799 Dutch.
-
Systematic review of high-cost patients' characteristics and healthcare utilisation.BMJ Open. 2018 Sep 8;8(9):e023113. doi: 10.1136/bmjopen-2018-023113. BMJ Open. 2018. PMID: 30196269 Free PMC article.
-
Characteristics and health care utilization among patients with chronic heart failure: a longitudinal claim database analysis.ESC Heart Fail. 2019 Dec;6(6):1243-1251. doi: 10.1002/ehf2.12512. Epub 2019 Sep 26. ESC Heart Fail. 2019. PMID: 31556246 Free PMC article.
-
Economic burden of paediatric-onset disabilities among young and middle-aged adults in the USA: a cohort study of privately insured beneficiaries.BMJ Open. 2019 Sep 3;9(9):e030490. doi: 10.1136/bmjopen-2019-030490. BMJ Open. 2019. PMID: 31481565 Free PMC article.
-
Prevalence and Medical Costs of Chronic Diseases Among Adult Medicaid Beneficiaries.Am J Prev Med. 2017 Dec;53(6S2):S143-S154. doi: 10.1016/j.amepre.2017.07.019. Am J Prev Med. 2017. PMID: 29153115 Free PMC article. Review.
Cited by
-
Patterns of healthcare resource utilization in patients with sarcoidosis: a cross-sectional study.Sarcoidosis Vasc Diffuse Lung Dis. 2020;37(3):e2020002. doi: 10.36141/svdld.v37i3.9261. Epub 2020 Sep 30. Sarcoidosis Vasc Diffuse Lung Dis. 2020. PMID: 33264377 Free PMC article.
-
The Impact of Payment Reforms on the Quality and Utilisation of Healthcare for Patients With Multimorbidity: A Systematic Review.Int J Integr Care. 2022 Feb 10;22(1):10. doi: 10.5334/ijic.5937. eCollection 2022 Jan-Mar. Int J Integr Care. 2022. PMID: 35221826 Free PMC article.
-
Characterizing Cross-Provincial High-Cost Patients in Rural China: Cross-Sectional Study.JMIR Public Health Surveill. 2025 Jun 11;11:e54234. doi: 10.2196/54234. JMIR Public Health Surveill. 2025. PMID: 40499037 Free PMC article.
-
Policy Versus Practice: Facilitators and Barriers of Chronic Care Integration in Dutch General Practice - a Survey Study.Int J Integr Care. 2024 Dec 18;24(4):13. doi: 10.5334/ijic.8443. eCollection 2024 Oct-Dec. Int J Integr Care. 2024. PMID: 39711993 Free PMC article.
-
A hospital care coordination team intervention for patients with multimorbidity: A practice-based, participatory pilot study.Chronic Illn. 2025 Mar;21(1):25-41. doi: 10.1177/17423953231196611. Epub 2023 Sep 6. Chronic Illn. 2025. PMID: 37670688 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases