

Development of Protective Immunity in New Zealand White Rabbits Challenged with Bacillus anthracis Spores and Treated with Antibiotics and Obiltoxaximab, a Monoclonal Antibody against Protective Antigen
- PMID: 29133571
- PMCID: PMC5786786
- DOI: 10.1128/AAC.01590-17
Development of Protective Immunity in New Zealand White Rabbits Challenged with Bacillus anthracis Spores and Treated with Antibiotics and Obiltoxaximab, a Monoclonal Antibody against Protective Antigen
Abstract
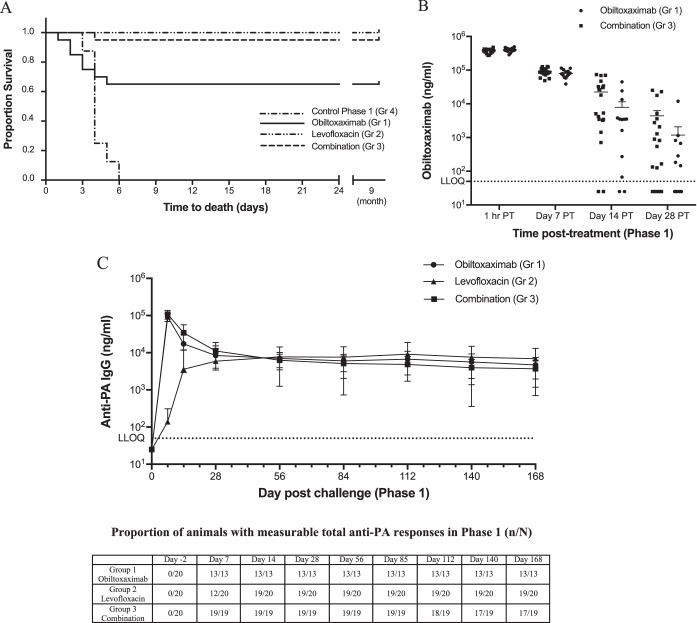
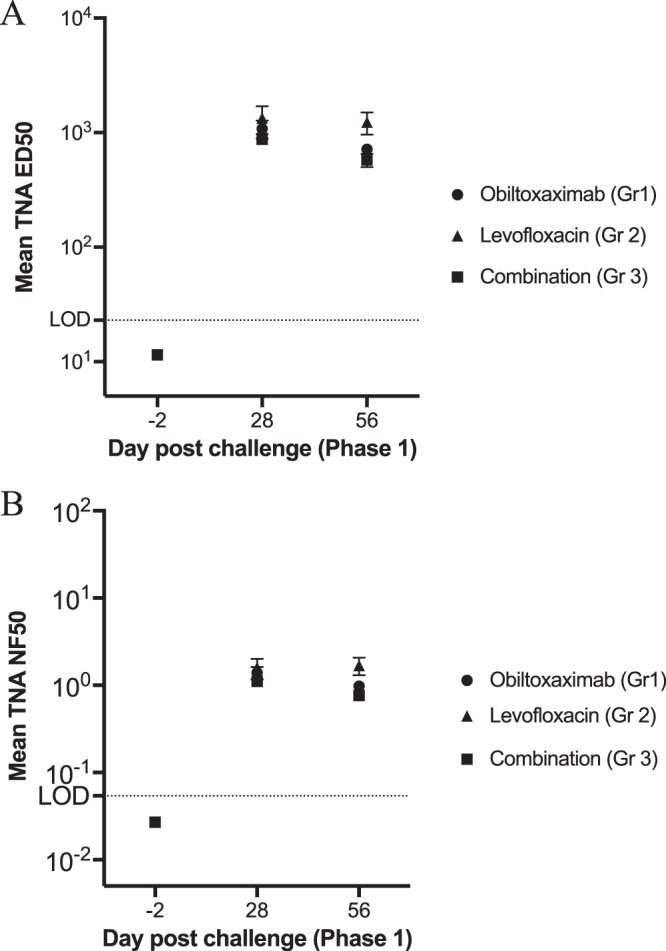
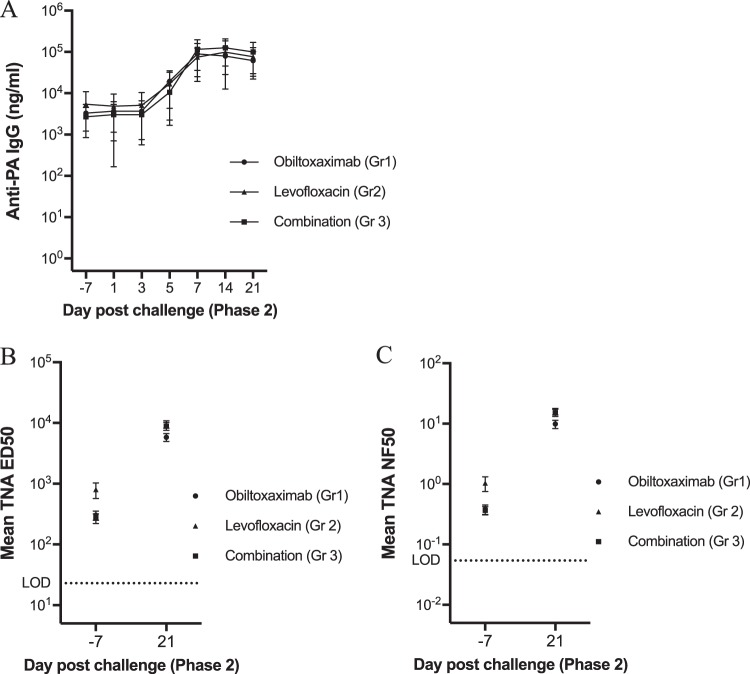
The recommended management of inhalational anthrax, a high-priority bioterrorist threat, includes antibiotics and antitoxins. Obiltoxaximab, a chimeric monoclonal antibody against anthrax protective antigen (PA), is licensed under the U.S. Food and Drug Administration's (FDA's) Animal Rule for the treatment of inhalational anthrax. Because of spore latency, disease reemergence after treatment cessation is a concern, and there is a need to understand the development of endogenous protective immune responses following antitoxin-containing anthrax treatment regimens. Here, acquired protective immunity was examined in New Zealand White (NZW) rabbits challenged with a targeted lethal dose of Bacillus anthracis spores and treated with antibiotics, obiltoxaximab, or a combination of both. Survivors of the primary challenge were rechallenged 9 months later and monitored for survival. Survival rates after primary and rechallenge for controls and animals treated with obiltoxaximab, levofloxacin, or a combination of both were 0, 65, 100, and 95%, and 0, 100, 95, and 89%, respectively. All surviving immune animals had circulating antibodies to PA and serum toxin-neutralizing titers prior to rechallenge. Following rechallenge, systemic bacteremia and toxemia were not detected in most animals, and the levels of circulating anti-PA IgG titers increased starting at 5 days postrechallenge. We conclude that treatment with obiltoxaximab, alone or combined with antibiotics, significantly improves the survival of rabbits that received a lethal inhalation B. anthracis spore challenge dose and does not interfere with the development of immunity. Survivors of primary challenge are protected against reexposure, have rare incidents of systemic bacteremia and toxemia, and have evidence of an anamnestic response.
Keywords: Bacillus anthracis; anthrax; antitoxin; immune memory; monoclonal antibodies; obiltoxaximab; protective antigen.
Copyright © 2018 Henning et al.
Figures

References
-
- Public Health Emergency Medical Countermeasures Enterprise (PHEMCE). 2016. 2016 Public Health Emergency Medical Countermeasures Enterprise (PHEMCE) strategy and implementation plan. Public Health Emergency Medical Countermeasures Enterprise, Washington, DC: https://www.phe.gov/Preparedness/mcm/phemce/Documents/2016-phemce-sip.pdf.
-
- Hendricks KA, Wright ME, Shadomy SV, Bradley JS, Morrow MG, Pavia AT, Rubinstein E, Holty JE, Messonnier NE, Smith TL, Pesik N, Treadwell TA, Bower WA, Workgroup on Anthrax Clinical Guidelines. 2014. Centers for Disease Control and Prevention expert panel meetings on prevention and treatment of anthrax in adults. Emerg Infect Dis 20. doi: 10.3201/eid2002.130687. - DOI - PMC - PubMed
-
- Jernigan DB, Raghunathan PL, Bell BP, Brechner R, Bresnitz EA, Butler JC, Cetron M, Cohen M, Doyle T, Fischer M, Greene C, Griffith KS, Guarner J, Hadler JL, Hayslett JA, Meyer R, Petersen LR, Phillips M, Pinner R, Popovic T, Quinn CP, Reefhuis J, Reissman D, Rosenstein N, Schuchat A, Shieh WJ, Siegal L, Swerdlow DL, Tenover FC, Traeger M, Ward JW, Weisfuse I, Wiersma S, Yeskey K, Zaki S, Ashford DA, Perkins BA, Ostroff S, Hughes J, Fleming D, Koplan JP, Gerberding JL, National Anthrax Epidemiologic Investigation Team. 2002. Investigation of bioterrorism-related anthrax, United States, 2001: epidemiologic findings. Emerg Infect Dis 8:1019–1028. doi: 10.3201/eid0810.020353. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
