

Pharmacokinetics and Safety of Amenamevir in Healthy Subjects: Analysis of Four Randomized Phase 1 Studies
- PMID: 29134426
- PMCID: PMC5709458
- DOI: 10.1007/s12325-017-0642-4
Pharmacokinetics and Safety of Amenamevir in Healthy Subjects: Analysis of Four Randomized Phase 1 Studies
Abstract
Introduction: Amenamevir (ASP2151) is a nonnucleoside antiherpesvirus compound available for the treatment of varicella-zoster virus infections. In this article we summarize the findings of four phase 1 studies in healthy participants.
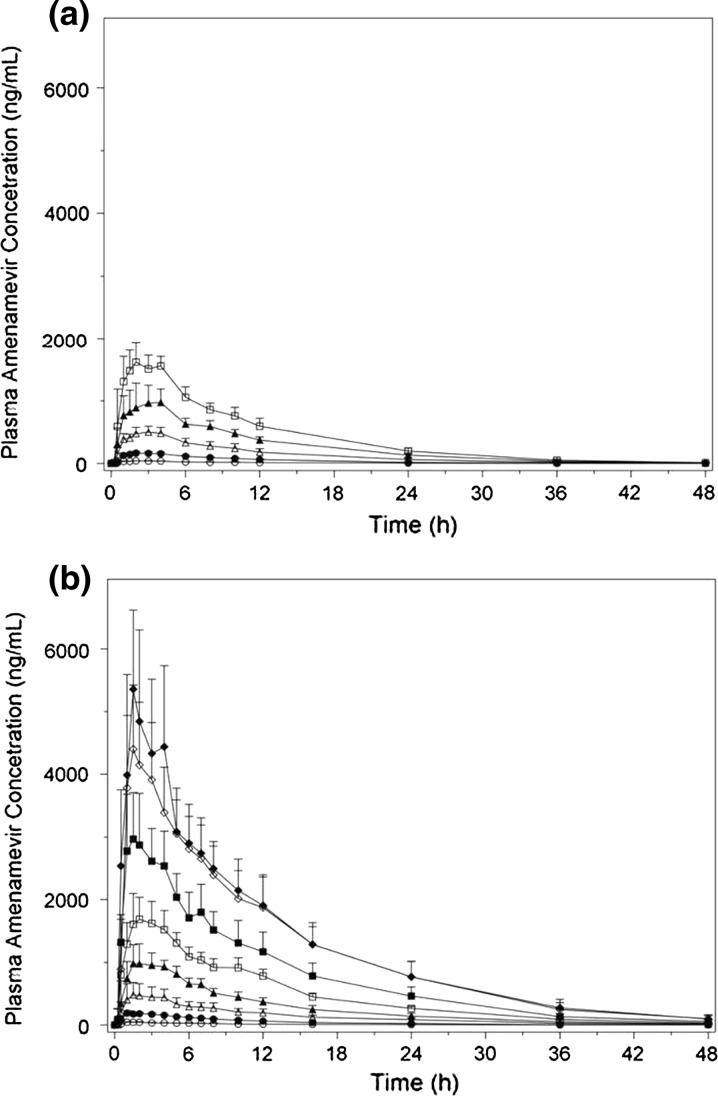
Methods: Four randomized phase 1 studies investigated the safety and pharmacokinetics of single and multiple doses of amenamevir, including the assessment of age group effect (nonelderly vs elderly), food effect, and the relative bioavailability of two formulations. Amenamevir was administered orally at various doses as a single dose (5-2400 mg) or daily (300 or 600 mg/day) for 7 days.
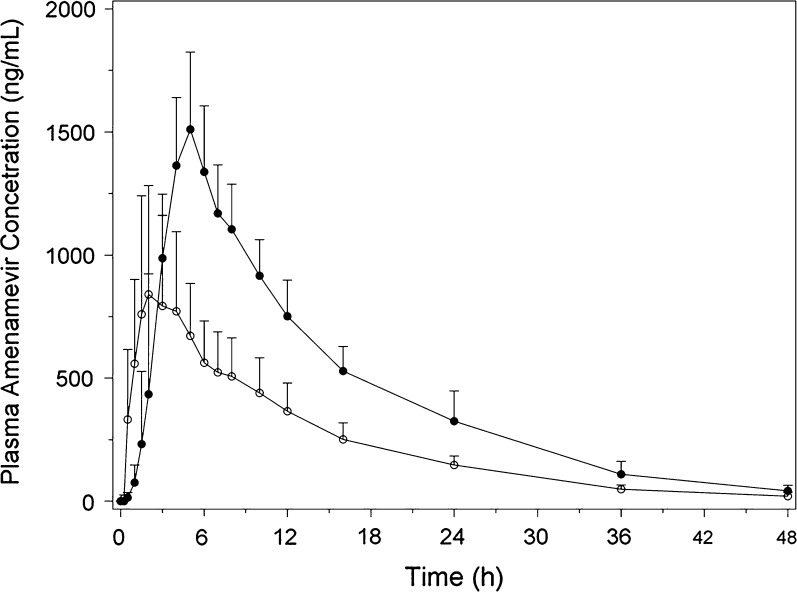
Results: Following single and multiple oral doses, amenamevir demonstrated a less than dose proportional increase in the pharmacokinetic parameters area under the plasma drug concentration versus time curve from time zero to infinity (AUCinf) and C max. After single and multiple oral 300-mg doses of amenamevir, no apparent differences in pharmacokinetics were observed between nonelderly and elderly participants. In contrast, with the amenamevir 600-mg dose both the area under the plasma drug concentration versus time curve from time zero to 24 h and C max were slightly increased and renal clearance was decreased in elderly participants. The pharmacokinetics of amenamevir was affected by food, with AUCinf increased by about 90%. In the bioavailability study, AUCinf and C max were slightly lower following tablet versus capsule administration (decreased by 14 and 12%, respectively), with relative bioavailability of 86%. The different amenamevir doses and formulations were safe and well tolerated; no deaths or serious adverse events were reported.
Conclusion: Amenamevir had less than dose proportional pharmacokinetic characteristics. Age may have an influence on amenamevir pharmacokinetics; however, the effect was considered minimal. The pharmacokinetics of amenamevir were affected by food, with AUCinf almost doubling when amenamevir was administered with food. The concentration versus time profile of the tablet was slightly lower than that of the capsule; the relative bioavailability of the tablet versus the capsule was 86%. Amenamevir was safe and well tolerated in the dose range investigated.
Funding: Astellas Pharma.
Trial registration: ClinicalTrials.gov identifiers NCT02852876 (15L-CL-002) and NCT02796118 (15L-CL-003).
Keywords: Amenamevir; Japanese participants; Pharmacokinetics; Safety; Varicella–zoster virus.
Figures

References
-
- Wareham DW, Breuer J. Herpes zoster. BMJ. 2007;334(7605):1211–1215. doi: 10.1136/bmj.39206.571042.AE. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
