

International Endocervical Adenocarcinoma Criteria and Classification (IECC): A New Pathogenetic Classification for Invasive Adenocarcinomas of the Endocervix
- PMID: 29135516
- PMCID: PMC5762258
- DOI: 10.1097/PAS.0000000000000986
International Endocervical Adenocarcinoma Criteria and Classification (IECC): A New Pathogenetic Classification for Invasive Adenocarcinomas of the Endocervix
Abstract
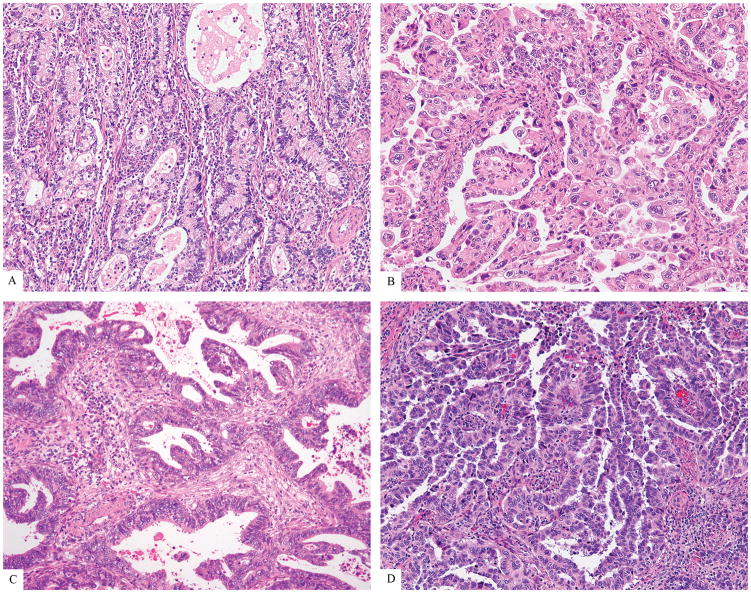
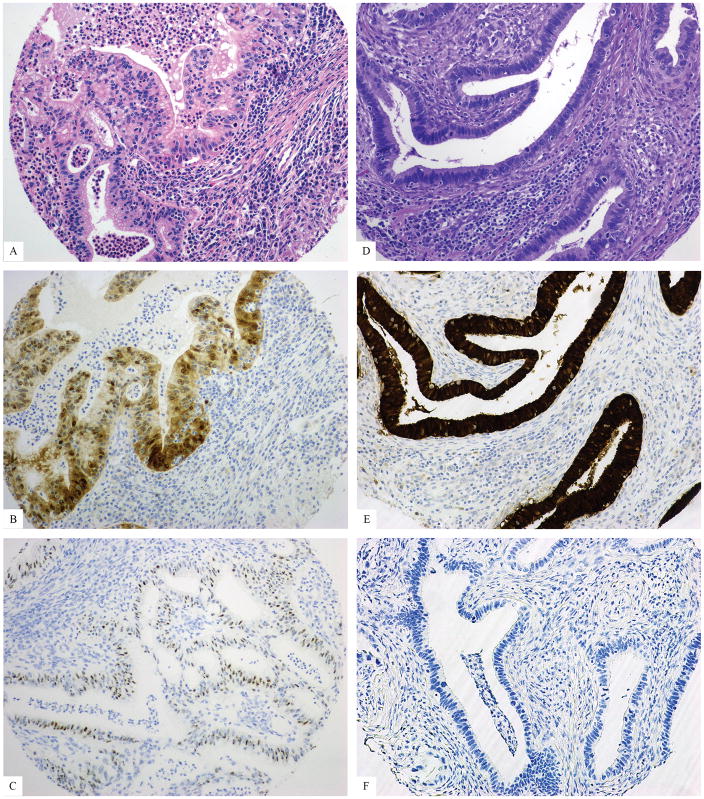
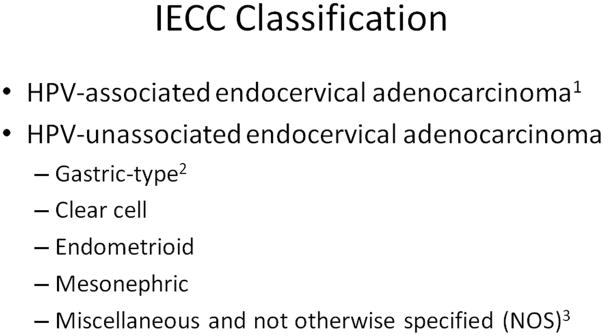
We sought to classify endocervical adenocarcinomas (ECAs) based on morphologic features linked to etiology (ie, human papillomavirus [HPV] infection), unlike the World Health Organization 2014 classification. The International Endocervical Adenocarcinoma Criteria and Classification (IECC criteria), described herein, distinguishes between human papillomavirus-associated adenocarcinoma (HPVA), recognized by the presence of luminal mitoses and apoptosis seen at scanning magnification, and no or limited HPVA features (nonhuman papillomavirus-associated adenocarcinoma [NHPVA]). HPVAs were then subcategorized based on cytoplasmic features (mostly to provide continuity with preexisting classification schemes), whereas NHPVAs were subclassified based on established criteria (ie, gastric-type, clear cell, etc.). Complete slide sets from 409 cases were collected from 7 institutions worldwide. Tissue microarrays representing 297 cases were constructed; immunohistochemistry (p16, p53, vimentin, progesterone receptor) and chromogenic in situ hybridization using an RNA-based probe set that recognizes 18 varieties of high-risk HPV were performed to validate IECC diagnoses. The 5 most common IECC diagnoses were usual-type (HPVA) (73% of cohort), gastric-type (NHPVA) (10%), mucinous adenocarcinoma of HPVA type, including intestinal, mucinous not otherwise specified, signet-ring, and invasive stratified mucin-producing carcinoma categories (9%), clear cell carcinoma (NHPVA) (3%) and adenocarcinoma, not otherwise specified (2%). Only 3 endometrioid carcinomas were recognized and all were NHPVA. When excluding cases thought to have suboptimal tissue processing, 90% and 95% of usual-type IECC cases overexpressed p16 and were HPV, whereas 37% and 3% of NHPVAs were p16 and HPV, respectively. The 1 HPV gastric-type carcinoma was found to have hybrid HPVA/NHPVA features on secondary review. NHPVA tumors were larger and occurred in significantly older patients, compared with HPVA tumors (P<0.001). The high-risk HPV chromogenic in situ hybridization probe set had superior sensitivity, specificity, and positive and negative predictive values (0.955, 0.968, 0.992, 0.833, respectively) compared with p16 immunohistochemistry (0.872, 0.632, 0.907, 0.545, respectively) to identify HPV-related usual carcinoma and mucinous carcinoma. IECC reliably segregates ECAs into HPVA and NHPVA types using morphology alone. This study confirms that usual-type ECAs are the most common type worldwide and that mucinous carcinomas comprise a mixture of HPVA and NHPVA, with gastric-type carcinoma being the major NHPVA type. Endometrioid and serous carcinomas of the endocervix are extraordinarily rare. Should clinical outcomes and genomic studies continue to support these findings, we recommend replacement of the World Health Organization 2014 criteria with the IECC 2017.
Conflict of interest statement
Figures





References
-
- Smith HO, Tiffany MF, Qualls CR, et al. The rising incidence of adenocarcinoma relative to squamous cell carcinoma of the uterine cervix in the United States—a 24-year population-based study. Gynecol Oncol. 2000;78:97–105. - PubMed
-
- Vesterinen E, Forss M, Nieminen U. Increase of cervical adenocarcinoma: a report of 520 cases of cervical carcinoma including 112 tumors with glandular elements. Gynecol Oncol. 1989;33:49–53. - PubMed
-
- An HJ, Kim KR, Kim IS, et al. Prevalence of human papillomavirus DNA in various histological subtypes of cervical adenocarcinoma: a population-based study. Mod Pathol. 2005;18:528–534. - PubMed
-
- Kurman RJ, Carcangiu ML, Herrington CS, Young RH. WHO Classification of tumors of female reproductive organs. 4. IARC. WHO Press; 2014.
-
- Young RH, Clement PB. Endocervical adenocarcinoma and its variants: their morphology and differential diagnosis. Histopathology. 2002;41:185–207. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
