

Assisted partner notification services are cost-effective for decreasing HIV burden in western Kenya
- PMID: 29135576
- PMCID: PMC5736414
- DOI: 10.1097/QAD.0000000000001697
Assisted partner notification services are cost-effective for decreasing HIV burden in western Kenya
Abstract
Background: Assisted partner services (aPS) or provider notification for sexual partners of persons diagnosed HIV positive can increase HIV testing and linkage in Sub-Saharan Africa and is a high yield strategy to identify HIV-positive persons. However, its cost-effectiveness is not well evaluated.
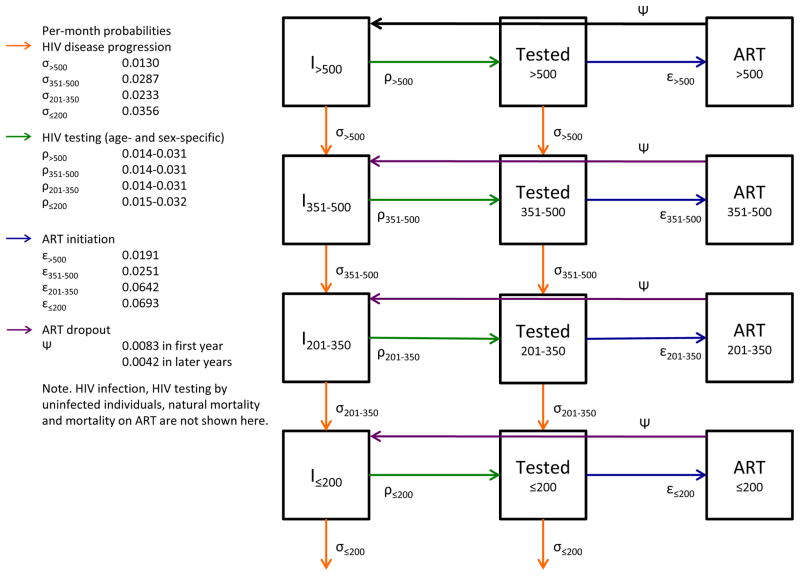
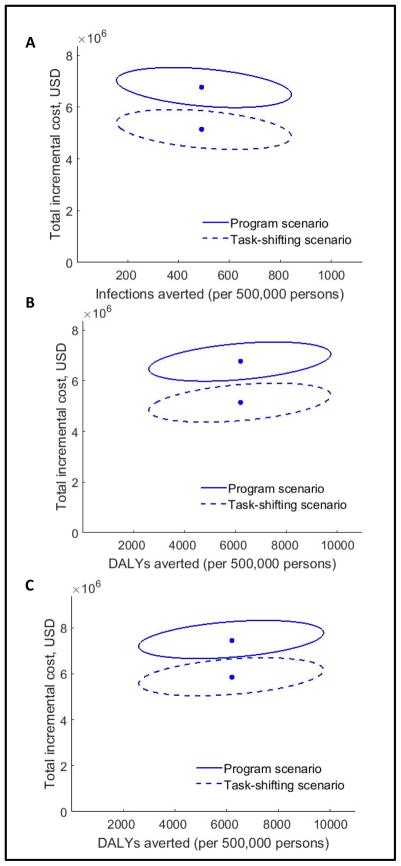
Methods: Using effectiveness and cost data from an aPS trial in Kenya, we parameterized an individual-based, dynamic HIV transmission model. We estimated costs for both a program scenario and a task-shifting scenario using community health workers to conduct the intervention. We simulated 200 cohorts of 500 000 individuals and projected the health and economic effects of scaling up aPS in a region of western Kenya (formerly Nyanza Province).
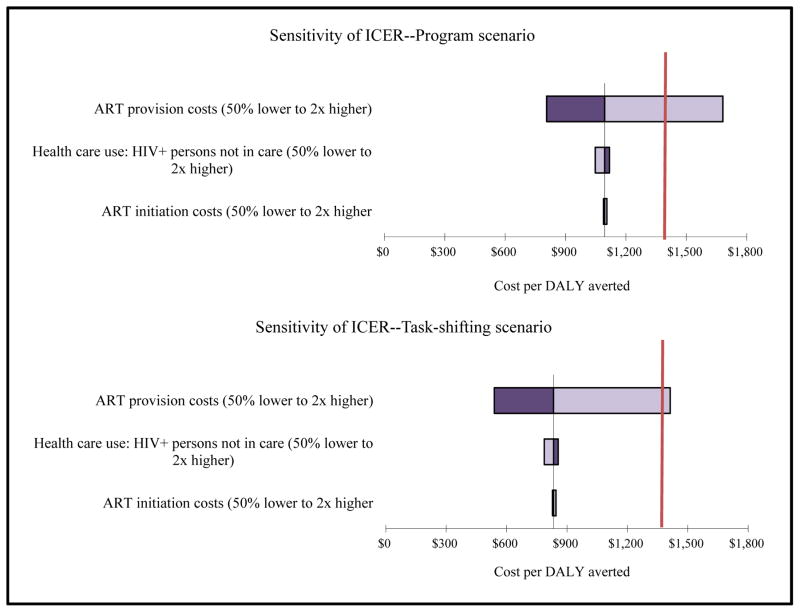
Findings: Over a 10-year time horizon with universal antiretroviral therapy (ART) initiation, implementing aPS in western Kenya was projected to reach 12.5% of the population and reduce incident HIV infections by 3.7%. In sexual partners receiving aPS, HIV-related deaths were reduced by 13.7%. The incremental cost-effectiveness ratio of aPS was $1094 (US dollars) (90% model variability $823-1619) and $833 (90% model variability $628-1224) per disability-adjusted life year averted under the program and task-shifting scenario, respectively. The incremental cost-effectiveness ratios for both scenarios fall below Kenya's gross domestic product per capita ($1358) and are therefore considered very cost-effective. Results were robust to varying healthcare costs, linkage to care rates, partner concurrency rates, and ART eligibility thresholds (≤350 cells/μl, ≤500 cells/μl, and universal ART).
Interpretation: APS is cost-effective for reducing HIV-related morbidity and mortality in western Kenya and similar settings. Task shifting can increase program affordability.
Conflict of interest statement
Conflicts of interest: The authors declare that they have no conflicts of interest.
Figures
References
-
- UNAIDS. [Accessed on 10/3/2015];The Gap Report. from: http://www.unaids.org/sites/default/files/media_asset/UNAIDS_Gap_report_....
-
- Marks G, Crepaz N, Janssen RS. Estimating sexual transmission of HIV from persons aware and unaware that they are infected with the virus in the USA. AIDS (London, England) 2006;20(10):1447–1450. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
