

Derivation and External Validation of Prediction Models for Advanced Chronic Kidney Disease Following Acute Kidney Injury
- PMID: 29136443
- PMCID: PMC5820711
- DOI: 10.1001/jama.2017.16326
Derivation and External Validation of Prediction Models for Advanced Chronic Kidney Disease Following Acute Kidney Injury
Abstract
Importance: Some patients will develop chronic kidney disease after a hospitalization with acute kidney injury; however, no risk-prediction tools have been developed to identify high-risk patients requiring follow-up.
Objective: To derive and validate predictive models for progression of acute kidney injury to advanced chronic kidney disease.
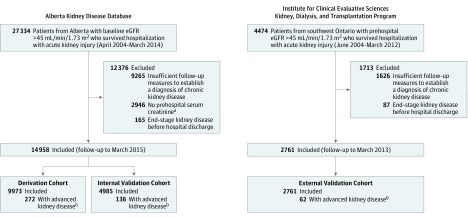
Design, setting, and participants: Data from 2 population-based cohorts of patients with a prehospitalization estimated glomerular filtration rate (eGFR) of more than 45 mL/min/1.73 m2 and who had survived hospitalization with acute kidney injury (defined by a serum creatinine increase during hospitalization > 0.3 mg/dL or > 50% of their prehospitalization baseline), were used to derive and validate multivariable prediction models. The risk models were derived from 9973 patients hospitalized in Alberta, Canada (April 2004-March 2014, with follow-up to March 2015). The risk models were externally validated with data from a cohort of 2761 patients hospitalized in Ontario, Canada (June 2004-March 2012, with follow-up to March 2013).
Exposures: Demographic, laboratory, and comorbidity variables measured prior to discharge.
Main outcomes and measures: Advanced chronic kidney disease was defined by a sustained reduction in eGFR less than 30 mL/min/1.73 m2 for at least 3 months during the year after discharge. All participants were followed up for up to 1 year.
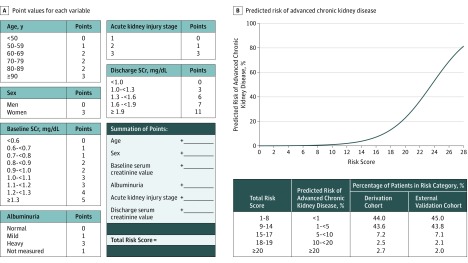
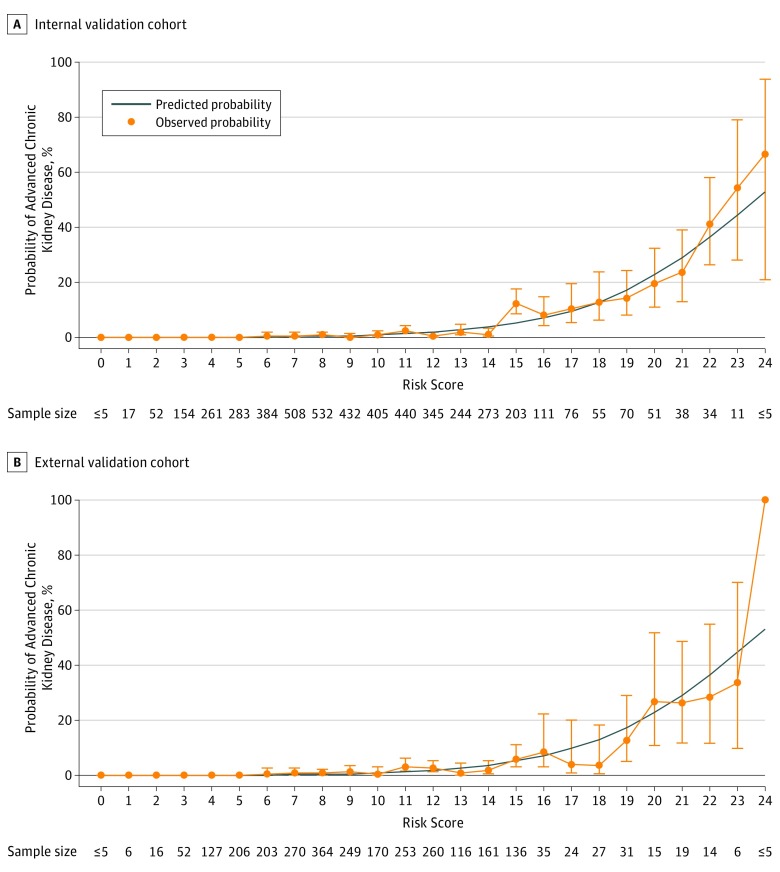
Results: The participants (mean [SD] age, 66 [15] years in the derivation and internal validation cohorts and 69 [11] years in the external validation cohort; 40%-43% women per cohort) had a mean (SD) baseline serum creatinine level of 1.0 (0.2) mg/dL and more than 20% had stage 2 or 3 acute kidney injury. Advanced chronic kidney disease developed in 408 (2.7%) of 9973 patients in the derivation cohort and 62 (2.2%) of 2761 patients in the external validation cohort. In the derivation cohort, 6 variables were independently associated with the outcome: older age, female sex, higher baseline serum creatinine value, albuminuria, greater severity of acute kidney injury, and higher serum creatinine value at discharge. In the external validation cohort, a multivariable model including these 6 variables had a C statistic of 0.81 (95% CI, 0.75-0.86) and improved discrimination and reclassification compared with reduced models that included age, sex, and discharge serum creatinine value alone (integrated discrimination improvement, 2.6%; 95% CI, 1.1%-4.0%; categorical net reclassification index, 13.5%; 95% CI, 1.9%-25.1%) or included age, sex, and acute kidney injury stage alone (integrated discrimination improvement, 8.0%; 95% CI, 5.1%-11.0%; categorical net reclassification index, 79.9%; 95% CI, 60.9%-98.9%).
Conclusions and relevance: A multivariable model using routine laboratory data was able to predict advanced chronic kidney disease following hospitalization with acute kidney injury. The utility of this model in clinical care requires further research.
Conflict of interest statement
Figures
References
-
- Ishani A, Nelson D, Clothier B, et al. . The magnitude of acute serum creatinine increase after cardiac surgery and the risk of chronic kidney disease, progression of kidney disease, and death. Arch Intern Med. 2011;171(3):226-233. - PubMed
-
- Kidney International Supplements KDIGO clinical practice guideline for acute kidney injury. http://www.kisupplements.org/issue/S2157-1716(12)X7200-9. Published March 2012. Accessed October 5, 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
