

The effect of interventions aiming to optimise the prescription of antibiotics in dental care-A systematic review
- PMID: 29136646
- PMCID: PMC5685629
- DOI: 10.1371/journal.pone.0188061
The effect of interventions aiming to optimise the prescription of antibiotics in dental care-A systematic review
Abstract
Background: Abundant evidence in dentistry suggests that antibiotics are prescribed despite the existence of guidelines aiming to reduce the development of antibiotic resistance. This review investigated (1) which type of interventions aiming to optimise prescription of antibiotics exist in dentistry, (2) the effect of these interventions and (3) the specific strengths and limitations of the studies reporting on these interventions.
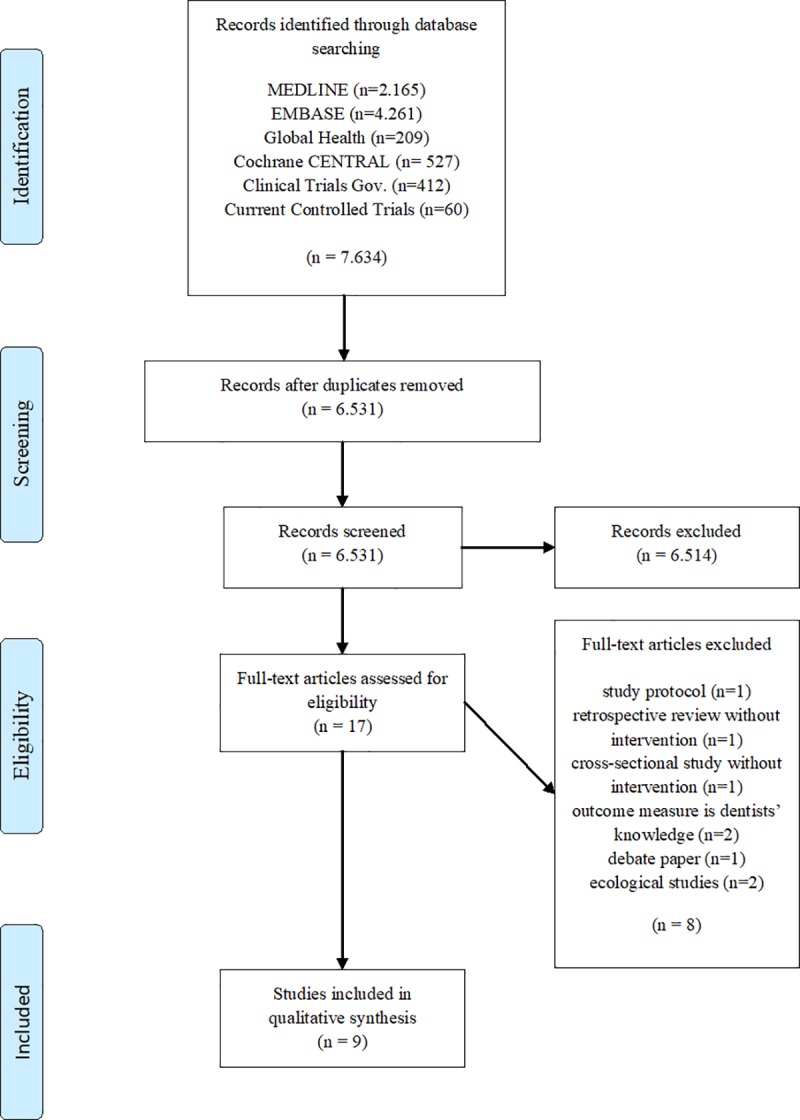
Method: Literature search was based on Medline, Embase, Global Health, Cochrane CENTRAL, ClinicalTrials.gov and Current Controlled Trials. Studies with one of the two primary outcomes were included: (1) The number of antibiotics prescribed and/or (2) the accuracy of the prescription, commonly measured as a percentage of adherence to local clinical guidelines.
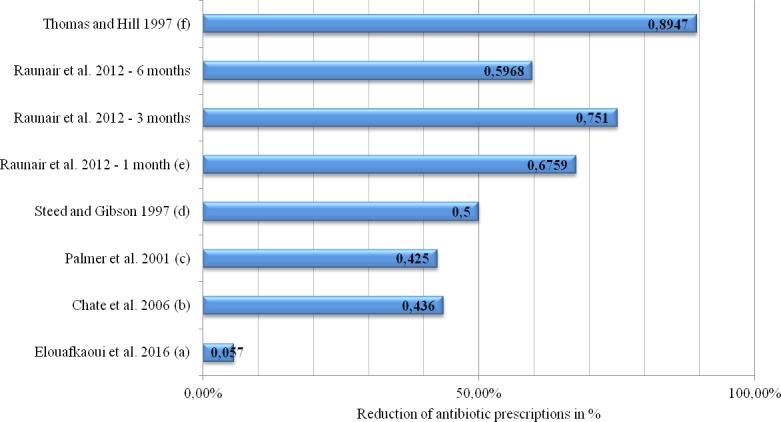
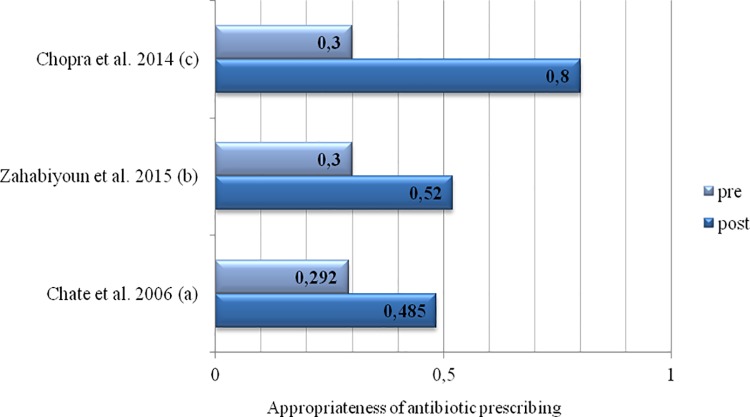
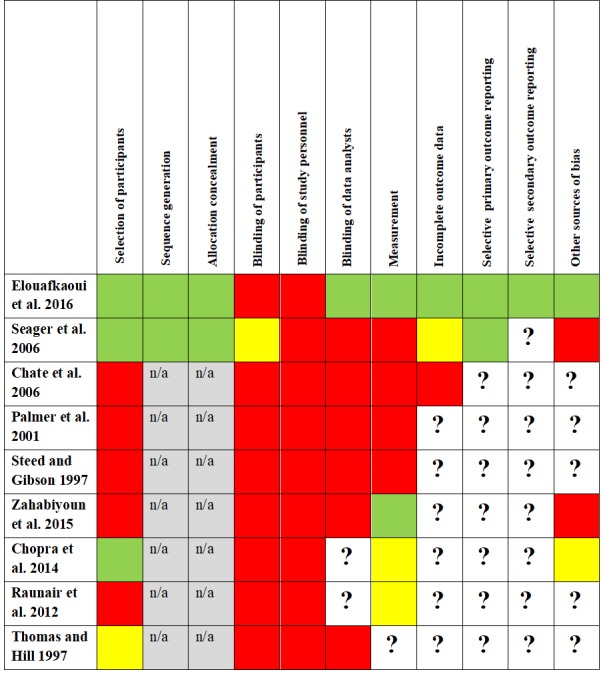
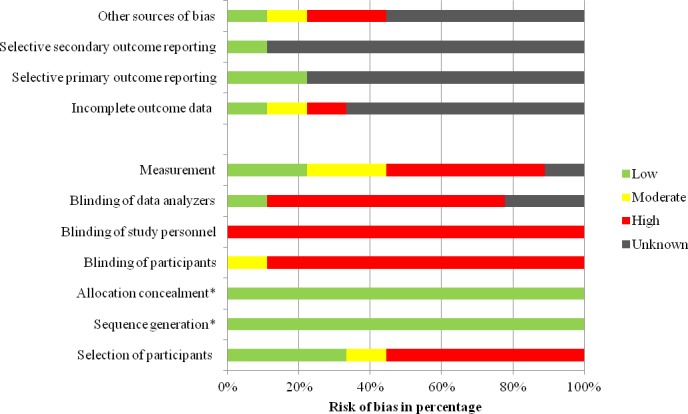
Results: Nine studies met these inclusion criteria. Five studies reported on the prescription of antibiotics in primary dental care and four studies focused on outpatient dental care. Interventions used in primary dental care included a combination of audit, feedback, education, local consensus, dissemination of guidelines and/or academic detailing. Trials in the outpatient setting made use of expert panel discussions, educational feedback on previous acts of prescribing, the dissemination of guidelines and the establishment of internal guidelines. All studies successfully reduced the number of antibiotics prescribed and/or increased the accuracy of the prescription. However, most studies were confounded by a high risk of selection bias, selective outcome reporting and high variance across study groups. In particular, information relating to study design and methodology was insufficient. Only three studies related the prescriptions to the number of patients treated with antibiotics.
Conclusions: This systematic review was able to offer conclusions which took the limitations of the investigated studies into account. Unfortunately, few studies could be included and many of these studies were confounded by a low quality of scientific reporting and lack of information regarding study methodology. High-quality research with objective and standardised outcome reporting, longer periods of follow-up, rigorous methodology and adequate standard of study reporting is urgently needed.
Conflict of interest statement
Figures
References
-
- Butler CC, Hood K, Verheij T, Little P, Melbye H, Nuttall J, et al. Variation in antibiotic prescribing and its impact on recovery in patients with acute cough in primary care: prospective study in 13 countries. Bmj. 2009;338:b2242 Epub 2009/06/25. doi: 10.1136/bmj.b2242 ; PubMed Central PMCID: PMCPMC3272656. - DOI - PMC - PubMed
-
- Gulliford MC, Moore MV, Little P, Hay AD, Fox R, Prevost AT, et al. Safety of reduced antibiotic prescribing for self limiting respiratory tract infections in primary care: cohort study using electronic health records. Bmj. 2016;354:i3410 Epub 2016/07/06. doi: 10.1136/bmj.i3410 ; PubMed Central PMCID: PMCPMC4933936. - DOI - PMC - PubMed
-
- Kenealy T, Arroll B. Antibiotics for the common cold and acute purulent rhinitis. Cochrane Library of Systematic Reviews; 2017. doi: 10.1002/14651858.CD000247.pub3 - DOI - PubMed
-
- Little P, Stuart B, Moore M, Coenen S, Butler CC, Godycki-Cwirko M, et al. Amoxicillin for acute lower-respiratory-tract infection in primary care when pneumonia is not suspected: a 12-country, randomised, placebo-controlled trial. The Lancet Infectious diseases. 2013;13(2):123–9. Epub 2012/12/26. doi: 10.1016/S1473-3099(12)70300-6 . - DOI - PubMed
-
- Price DB, Honeybourne D, Little P, Mayon-White RT, Read RC, Thomas M, et al. Community-acquired pneumonia mortality: a potential link to antibiotic prescribing trends in general practice. Respir Med. 2004;98(1):17–24. Epub 2004/02/13. . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
