

Tuberculosis presenting as isolated bronchonodal fistula in a patient with systemic lupus erythematosus: Case report
- PMID: 29137108
- PMCID: PMC5690801
- DOI: 10.1097/MD.0000000000008764
Tuberculosis presenting as isolated bronchonodal fistula in a patient with systemic lupus erythematosus: Case report
Abstract
Rationale: Lymph node is a preferred site for extrapulmonary tuberculosis (TB). In the thorax, mediastinal tuberculous lymph nodes can erode adjacent structures such as heart, aorta, and esophagus, forming fistula, and causing fatal consequences. However, tuberculous bronchonodal fistula as a complication of lymph node TB in adults is rarely known in terms of imaging or clinical findings. Here, a case of isolated tuberculous bronchonodal fistula appearing as the first presentation of TB in a 74-year-old male with systemic lupus erythematosus (SLE) is reported.
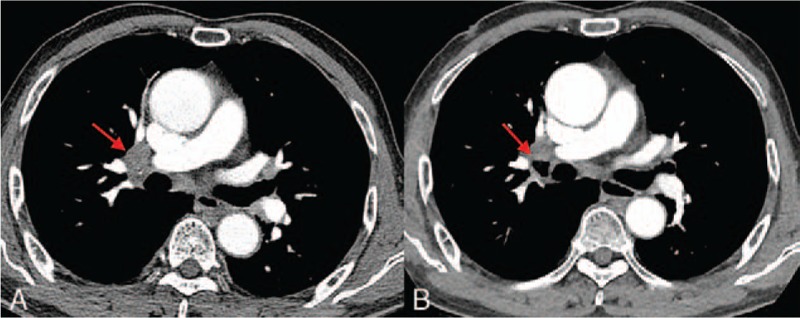
Patient concern: A 74-year-old male with SLE visited the hospital with dry cough. In family history, his son was treated for pulmonary TB 9 years previously. Laboratory test revealed increased C-reactive protein level and erythrocyte sedimentation rate. Chest computed tomography (CT) scan revealed a necrotic lymph node in the right hilar area connected to the inferior wall of the right upper lobe bronchus and the lateral wall of bronchus intermedius.
Diagnoses: On bronchoscopy performed under guidance of 3-dimensionally reconstructed CT image, fistula formation between the right hilar lymph node and 2 bronchi (the right upper lobe and intermediate bronchus) was confirmed. Sputum culture revealed growth of Mycobacterium tuberculosis.
Intervention: Anti-TB medication with isoniazid, ethambutol, pyrazinamide, and moxifloxacin for 9 months.
Outcome: The patient's symptom was gradually improved. Follow-up bronchoscopy performed at 3 months after starting the medication revealed decreased size of the fistula.
Lessons: This is a rare case of bronchonodal fistula appearing as the first presentation of TB in a 74-year-old male patient with SLE. CT provided useful information regarding the origin and progress of the disease.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures


References
-
- Yun JE, Lee SW, Kim TH, et al. The incidence and clinical characteristics of Mycobacterium tuberculosis infection among systemic lupus erythematosus and rheumatoid arthritis patients in Korea. Clin Exp Rheumatol 2002;20:127–32. - PubMed
-
- Woodring JH, Vandiviere HM, Lee C. Intrathoracic lymphadenopathy in postprimary tuberculosis. South Med J 1988;81:992–7. - PubMed
-
- Krishnan B, Shaukat A, Chakravorty I. Fatal haemoptysis in a young man with tuberculous mediastinal lymphadenitis. A case report and review of the literature. Respiration 2009;77:333–6. - PubMed
-
- Kasilingam SK, Sinha N, Kambar V, et al. Mediastinal tubercular lymph node eroding into pericardium causing acute pyopericardium and cardiac tamponade. Trop Doct 2014;44:114–5. - PubMed
-
- Erlank A, Goussard P, Andronikou S, et al. Oesophageal perforation as a complication of primary pulmonary tuberculous lymphadenopathy in children. Pediatr Radiol 2007;37:636–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
