

Mortality and pulmonary outcomes of extremely preterm infants exposed to antenatal corticosteroids
- PMID: 29138031
- PMCID: PMC5842434
- DOI: 10.1016/j.ajog.2017.11.554
Mortality and pulmonary outcomes of extremely preterm infants exposed to antenatal corticosteroids
Abstract
Background: Antenatal corticosteroids are given primarily to induce fetal lung maturation but results from meta-analyses of randomized controlled trials have not shown mortality or pulmonary benefits for extremely preterm infants although these are the infants most at risk of mortality and pulmonary disease.
Objective: We sought to determine if exposure to antenatal corticosteroids is associated with a lower rate of death and pulmonary morbidities by 36 weeks' postmenstrual age.
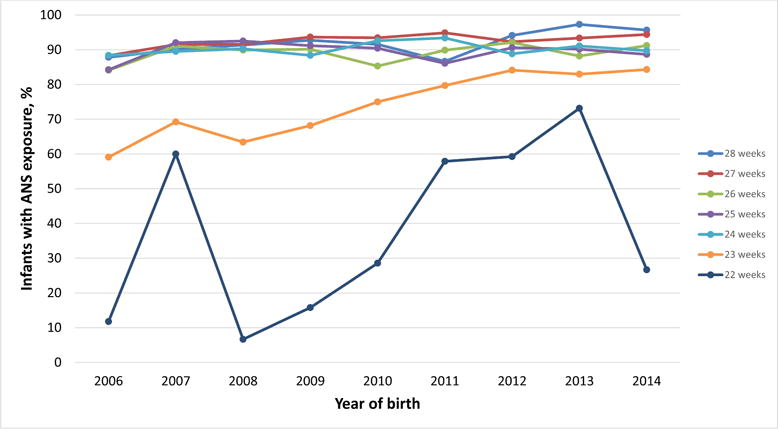
Study design: Prospectively collected data on 11,022 infants 22 0/7 to 28 6/7 weeks' gestational age with a birthweight of ≥401 g born from Jan. 1, 2006, through Dec. 31, 2014, were analyzed. The rate of death and the rate of physiologic bronchopulmonary dysplasia by 36 weeks' postmenstrual age were analyzed by level of exposure to antenatal corticosteroids using models adjusted for maternal variables, infant variables, center, and epoch.
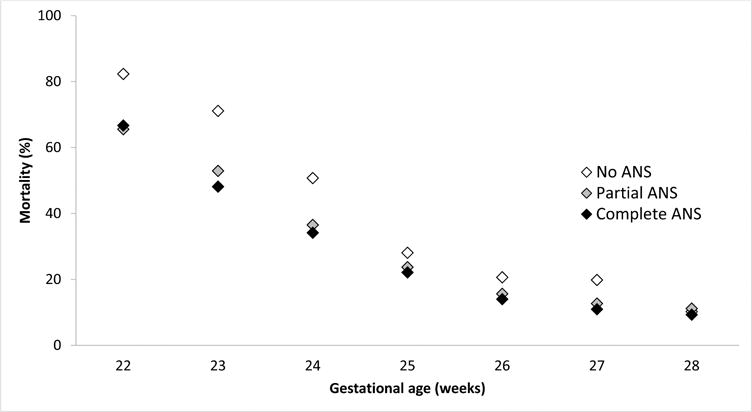
Results: Infants exposed to any antenatal corticosteroids had a lower rate of death (2193/9670 [22.7%]) compared to infants without exposure (540/1302 [41.5%]) (adjusted relative risk, 0.71; 95% confidence interval, 0.65-0.76; P < .0001). Infants exposed to a partial course of antenatal corticosteroids also had a lower rate of death (654/2520 [26.0%]) compared to infants without exposure (540/1302 [41.5%]); (adjusted relative risk, 0.77; 95% confidence interval, 0.70-0.85; P < .0001). In an analysis by each week of gestation, infants exposed to a complete course of antenatal corticosteroids had lower mortality before discharge compared to infants without exposure at each week from 23-27 weeks' gestation and infants exposed to a partial course of antenatal corticosteroids had lower mortality at 23, 24, and 26 weeks' gestation. Rates of bronchopulmonary dysplasia in survivors did not differ by antenatal corticosteroid exposure. The rate of death due to respiratory distress syndrome, the rate of surfactant use, and the rate of mechanical ventilation were lower in infants exposed to any antenatal corticosteroids compared to infants without exposure.
Conclusion: Among infants 22-28 weeks' gestational age, any or partial antenatal exposure to corticosteroids compared to no exposure is associated with a lower rate of death while the rate of bronchopulmonary dysplasia in survivors did not differ.
Keywords: antenatal corticosteroids; bronchopulmonary dysplasia; infant; intracranial hemorrhage; mechanical ventilation; morbidity; mortality; necrotizing enterocolitis; neonatal; newborn; patent ductus arteriosus; periventricular leukomalacia; pneumothorax; preterm; pulmonary; pulmonary hemorrhage; respiratory distress syndrome; respiratory support; sepsis; surfactant.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
-
- Roberts D, Dalziel S. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006;3:CD004454. - PubMed
-
- Onland W, de Laat MW, Mol BW, Offringa M. Effects of antenatal corticosteroids given prior to 26 weeks’ gestation: a systematic review of randomized controlled trials. Am J Perinatol. 2011;28(1):33–44. - PubMed
-
- Wong D, Abdel-Latif M, Kent A, NICUS Network Antenatal steroid exposure and outcomes of very premature infants: a regional cohort study. Arch Dis Child Fetal Neonatal Ed. 2014;99(1):F12–20. - PubMed
-
- Mori R, Kusuda S, Fujimura M, Neonatal Research Network Antenatal corticosteroids promote survival of extremely preterm infants born at 22 to 23 weeks of gestation. J Pediatr. 2011;159(1):110–114. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
- U10 HD021385/HD/NICHD NIH HHS/United States
- U10 HD053119/HD/NICHD NIH HHS/United States
- U10 HD021364/HD/NICHD NIH HHS/United States
- UG1 HD040689/HD/NICHD NIH HHS/United States
- UG1 HD034216/HD/NICHD NIH HHS/United States
- U10 HD027871/HD/NICHD NIH HHS/United States
- UG1 HD027904/HD/NICHD NIH HHS/United States
- UG1 HD021364/HD/NICHD NIH HHS/United States
- UG1 HD027880/HD/NICHD NIH HHS/United States
- U10 HD068284/HD/NICHD NIH HHS/United States
- U10 HD068278/HD/NICHD NIH HHS/United States
- UG1 HD027851/HD/NICHD NIH HHS/United States
- U10 HD040498/HD/NICHD NIH HHS/United States
- U10 HD027856/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- UG1 HD087226/HD/NICHD NIH HHS/United States
- U10 HD053124/HD/NICHD NIH HHS/United States
- U10 HD027880/HD/NICHD NIH HHS/United States
- UG1 HD027853/HD/NICHD NIH HHS/United States
- U10 HD040521/HD/NICHD NIH HHS/United States
- U10 HD053109/HD/NICHD NIH HHS/United States
- T32 HS013852/HS/AHRQ HHS/United States
- U10 HD040461/HD/NICHD NIH HHS/United States
- M01 RR016587/RR/NCRR NIH HHS/United States
- U10 HD040689/HD/NICHD NIH HHS/United States
- U10 HD040492/HD/NICHD NIH HHS/United States
- U10 HD027853/HD/NICHD NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- U10 HD021397/HD/NICHD NIH HHS/United States
- U10 HD068244/HD/NICHD NIH HHS/United States
- U10 HD068263/HD/NICHD NIH HHS/United States
- U10 HD068270/HD/NICHD NIH HHS/United States
- M01 RR007122/RR/NCRR NIH HHS/United States
- U10 HD027851/HD/NICHD NIH HHS/United States
- U10 HD034216/HD/NICHD NIH HHS/United States
- U10 HD036790/HD/NICHD NIH HHS/United States
- M01 RR006022/RR/NCRR NIH HHS/United States
- U10 HD053089/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
