

Comparative clinical effectiveness and cost effectiveness of endovascular strategy v open repair for ruptured abdominal aortic aneurysm: three year results of the IMPROVE randomised trial
- PMID: 29138135
- PMCID: PMC5682594
- DOI: 10.1136/bmj.j4859
Comparative clinical effectiveness and cost effectiveness of endovascular strategy v open repair for ruptured abdominal aortic aneurysm: three year results of the IMPROVE randomised trial
Abstract
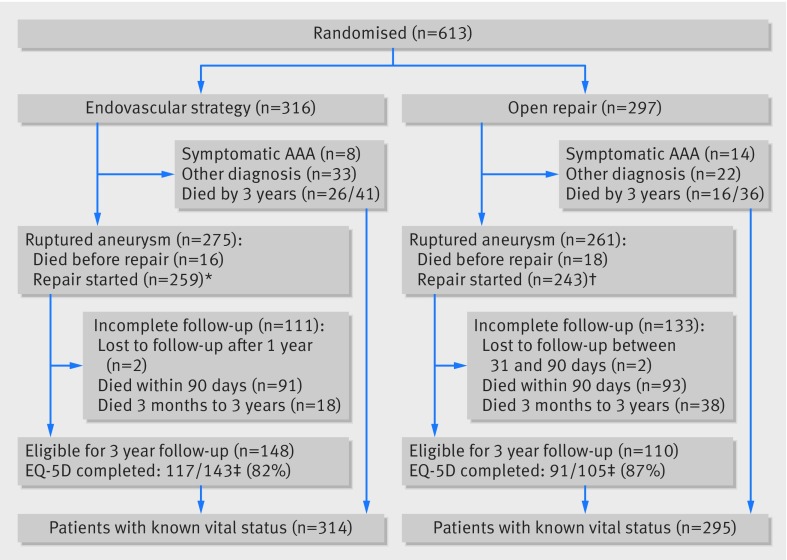
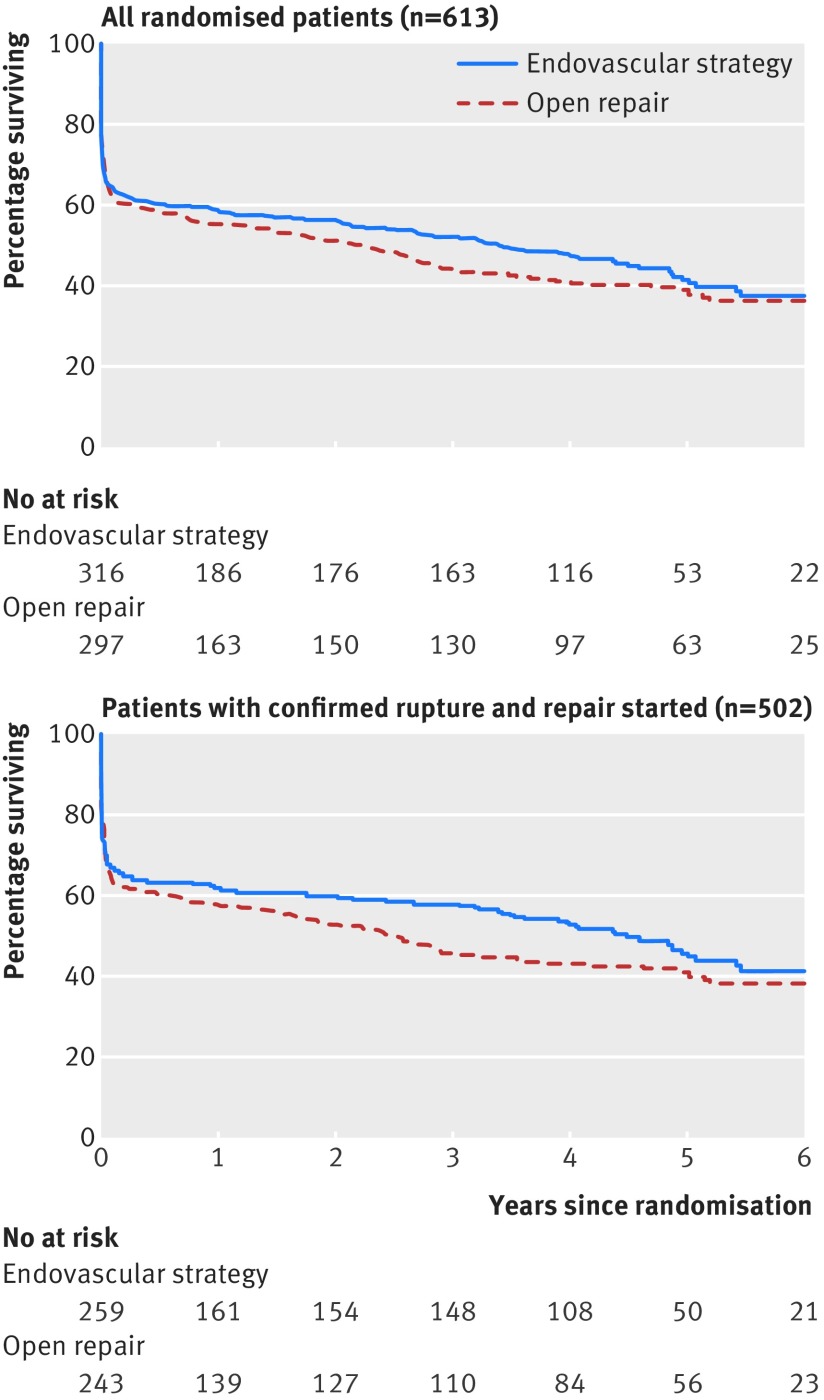
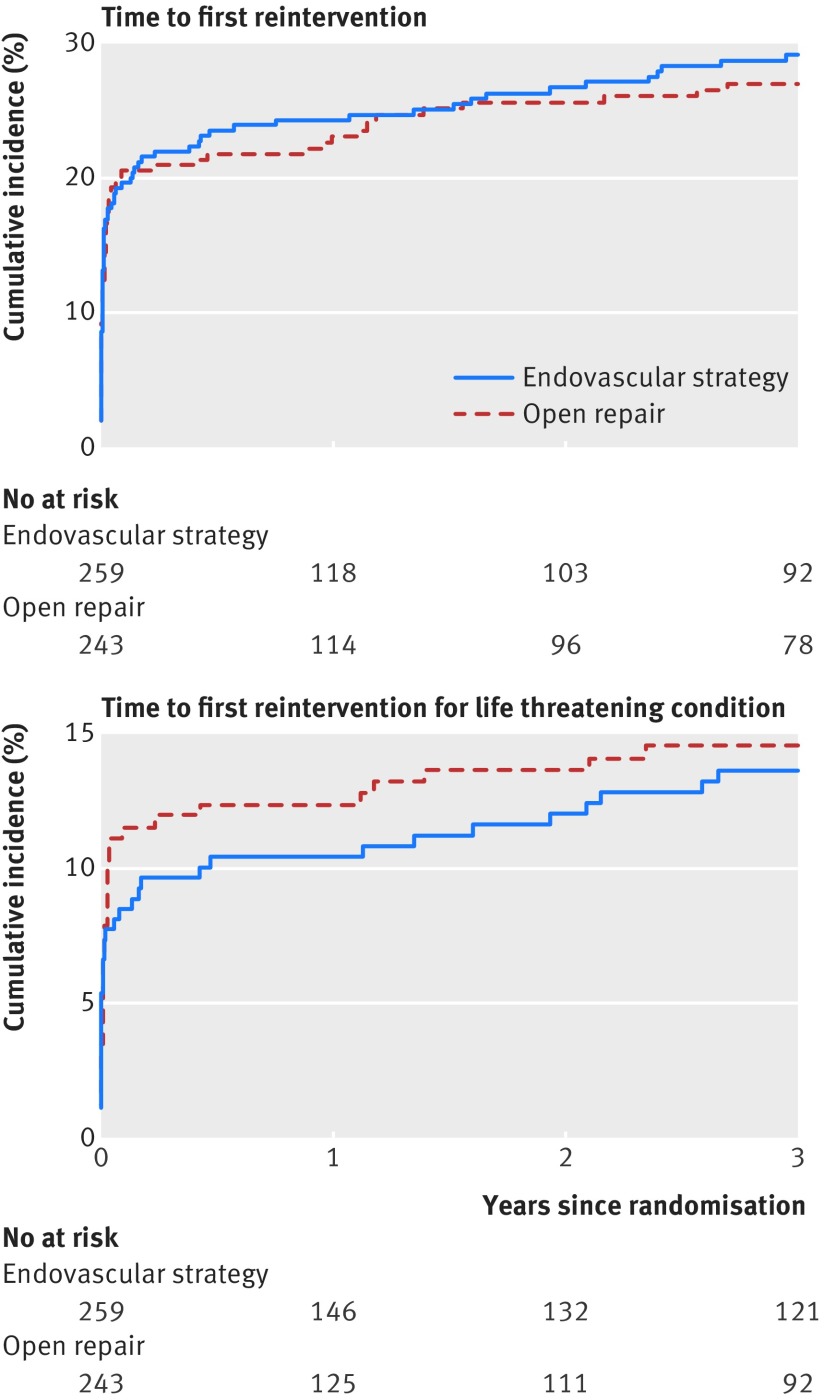
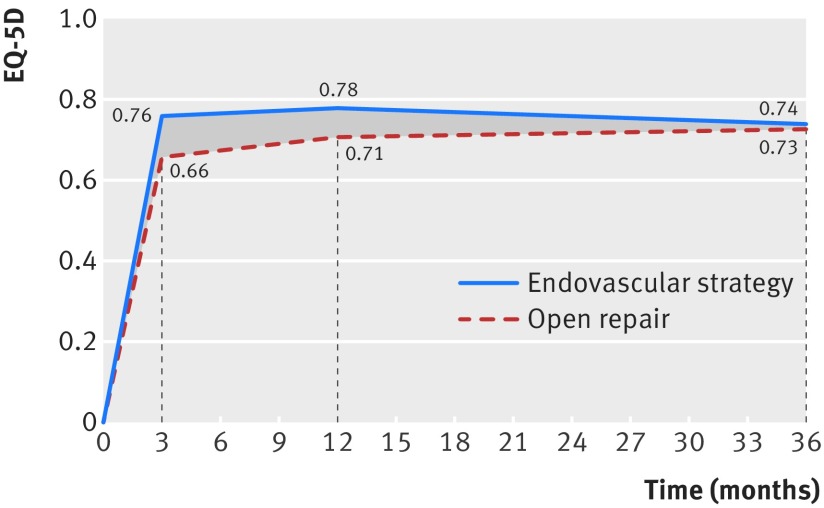
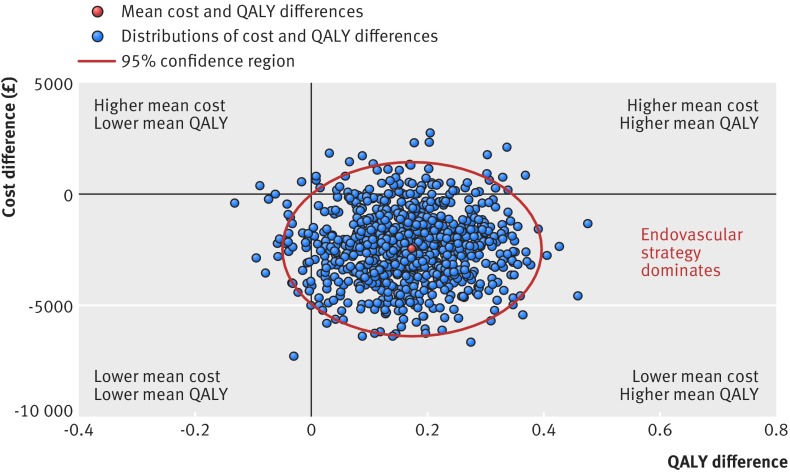
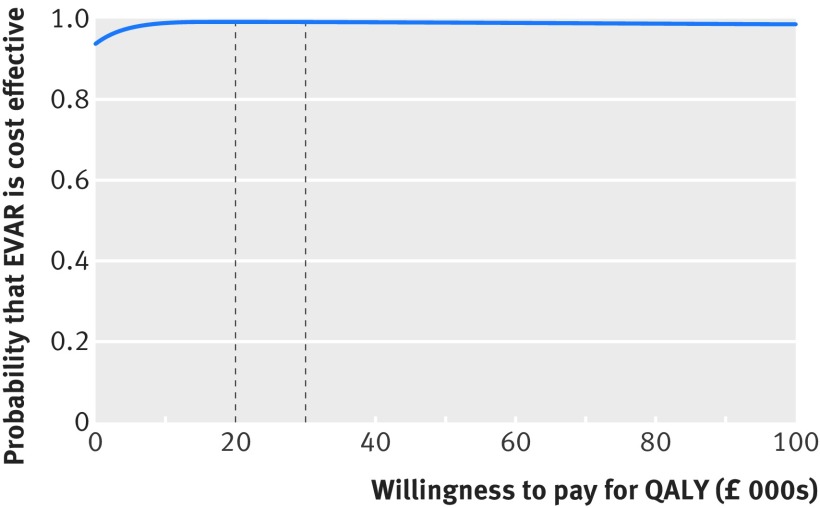
Objective To assess the three year clinical outcomes and cost effectiveness of a strategy of endovascular repair (if aortic morphology is suitable, open repair if not) versus open repair for patients with suspected ruptured abdominal aortic aneurysm.Design Randomised controlled trial.Setting 30 vascular centres (29 in UK, one in Canada), 2009-16.Participants 613 eligible patients (480 men) with a clinical diagnosis of ruptured aneurysm, of whom 502 underwent emergency repair for rupture.Interventions 316 patients were randomised to an endovascular strategy (275 with confirmed rupture) and 297 to open repair (261 with confirmed rupture).Main outcome measures Mortality, with reinterventions after aneurysm repair, quality of life, and hospital costs to three years as secondary measures.Results The maximum follow-up for mortality was 7.1 years, with two patients in each group lost to follow-up by three years. After similar mortality by 90 days, in the mid-term (three months to three years) there were fewer deaths in the endovascular than the open repair group (hazard ratio 0.57, 95% confidence interval 0.36 to 0.90), leading to lower mortality at three years (48% v 56%), but by seven years mortality was about 60% in each group (hazard ratio 0.92, 0.75 to 1.13). Results for the 502 patients with repaired ruptures were more pronounced: three year mortality was lower in the endovascular strategy group (42% v 54%; odds ratio 0.62, 0.43 to 0.88), but after seven years there was no clear difference between the groups (hazard ratio 0.86, 0.68 to 1.08). Reintervention rates up to three years were not significantly different between the randomised groups (hazard ratio 1.02, 0.79 to 1.32); the initial rapid rate of reinterventions was followed by a much slower mid-term reintervention rate in both groups. The early higher average quality of life in the endovascular strategy versus open repair group, coupled with the lower mortality at three years, led to a gain in average quality adjusted life years (QALYs) at three years of 0.17 (95% confidence interval 0.00 to 0.33). The endovascular strategy group spent fewer days in hospital and had lower average costs of -£2605 (95% confidence interval -£5966 to £702) (about €2813; $3439). The probability that the endovascular strategy is cost effective was >90% at all levels of willingness to pay for a QALY gain.Conclusions At three years, compared with open repair, an endovascular strategy for suspected ruptured abdominal aortic aneurysm was associated with a survival advantage, a gain in QALYs, similar levels of reintervention, and reduced costs, and this strategy was cost effective. These findings support the increasing use of an endovascular strategy, with wider availability of emergency endovascular repair.Trial registration Current Controlled Trials ISRCTN48334791; ClinicalTrials NCT00746122.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work;no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Endovascular or open repair for ruptured abdominal aortic aneurysm?BMJ. 2017 Nov 14;359:j5170. doi: 10.1136/bmj.j5170. BMJ. 2017. PMID: 29138183 Free PMC article.
References
-
- Sweeting MJ, Balm R, Desgranges P, Ulug P, Powell JT. Ruptured Aneurysm Trialists. Individual-patient meta-analysis of three randomized trials comparing endovascular versus open repair for ruptured abdominal aortic aneurysm. Br J Surg 2015;102:1229-39. 10.1002/bjs.9852 pmid:26104471. - DOI - PMC - PubMed
-
- Powell JT, Sweeting MJ, Thompson MM, et al. IMPROVE Trial Investigators. Endovascular or open repair strategy for ruptured abdominal aortic aneurysm: 30 day outcomes from IMPROVE randomised trial. BMJ 2014;348:f7661 10.1136/bmj.f7661 pmid:24418950. - DOI - PubMed
-
- Björck M. Surgery for ruptured abdominal aortic aneurysm. BMJ 2014;348:g95 10.1136/bmj.g95 pmid:24418688. - DOI - PubMed
-
- Mastracci TM, Garrido-Olivares L, Cinà CS, Clase CM. Endovascular repair of ruptured abdominal aortic aneurysms: a systematic review and meta-analysis. J Vasc Surg 2008;47:214-21. 10.1016/j.jvs.2007.07.052 pmid:18178478. - DOI - PubMed
-
- van Beek SC, Conijn AP, Koelemay MJ, Balm R. Editor’s Choice - Endovascular aneurysm repair versus open repair for patients with a ruptured abdominal aortic aneurysm: a systematic review and meta-analysis of short-term survival. Eur J Vasc Endovasc Surg 2014;47:593-602. 10.1016/j.ejvs.2014.03.003 pmid:24746873. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical