

Impact of Excessive Weight Gain on Cardiovascular Outcomes in Type 1 Diabetes: Results From the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study
- PMID: 29138273
- PMCID: PMC5711332
- DOI: 10.2337/dc16-2523
Impact of Excessive Weight Gain on Cardiovascular Outcomes in Type 1 Diabetes: Results From the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study
Abstract
Objective: Intensive treatment (INT) of type 1 diabetes reduces the incidence of cardiovascular disease (CVD) events compared with conventional treatment (CONV), but it also results in more weight gain. Our objective was to examine whether excessive weight gain from INT of type 1 diabetes is independently associated with subsequent CVD events.
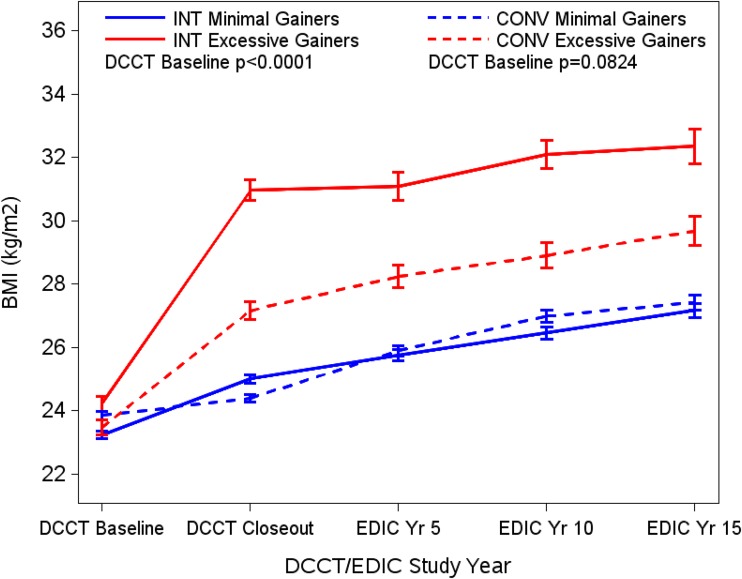
Research design and methods: Quartiles (Q) of weight gain in 1,213 participants aged 18 years and older at enrollment in the Diabetes Control and Complications Trial (DCCT) were determined within randomized treatment groups (INT vs. CONV) using change in BMI from baseline to the closeout DCCT visits. Effects of this weight gain on CVD risk factors and outcomes during an additional 20 years of observational follow-up were then determined.
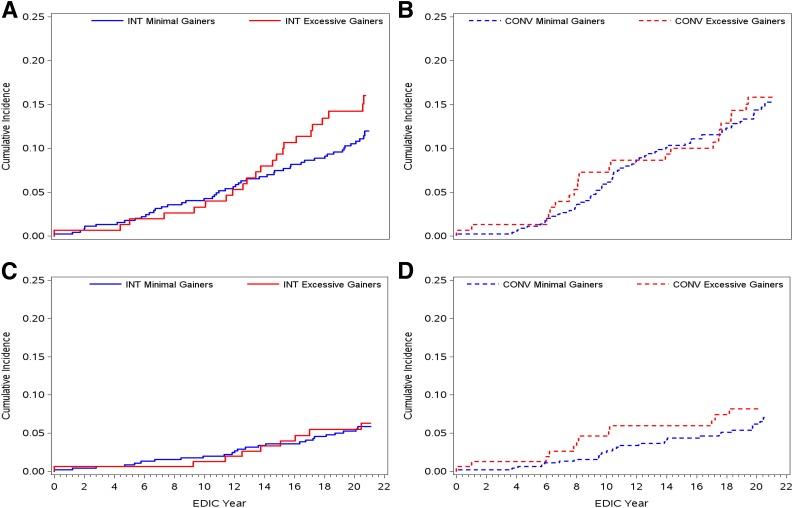
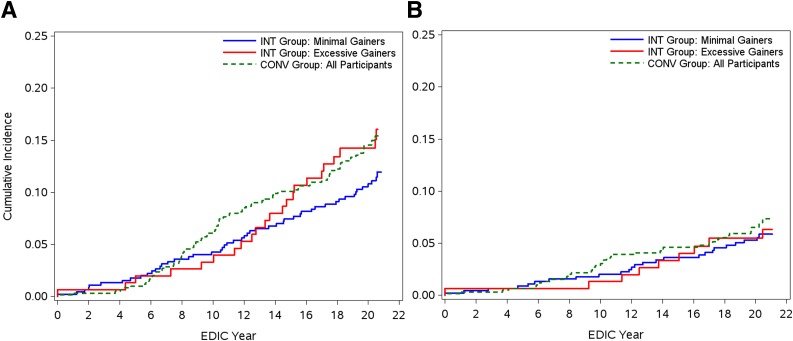
Results: The Q4 INT group experienced greater proportional weight gain (median change in BMI, 6.08 kg/m2), increases in CVD risk factors, and need for medications for hypertension and lipids compared with the Q1-3 INT and comparable CONV groups. Over a mean of 26 years of follow-up, the numbers of major and total CVD events were not statistically different in Q4 compared with Q1-3 of either the INT or CONV group. By year 14, however, the incident CVD event curve became significantly higher in the Q4 INT group than in the Q1-3 INT groups (P = 0.024) and was similar to that for the CONV group.
Conclusions: For the first 13 years after DCCT, INT for type 1 diabetes reduced macrovascular events compared with CONV, even when excessive weight gain occurred. After this, total CVD events significantly increased in the Q4 INT group, becoming equivalent to those in the CONV group. Longer follow-up is needed to determine whether this trend continues and results in more major CVD events.
Trial registration: ClinicalTrials.gov NCT00360815 NCT00360893.
© 2017 by the American Diabetes Association.
Figures
References
-
- Nathan DM, Cleary PA, Backlund JY, et al. .; Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group . Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med 2005;353:2643–2653 - PMC - PubMed
-
- Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) Study Research Group Intensive diabetes treatment and cardiovascular outcomes in type 1 diabetes: the DCCT/EDIC study 30-year follow-up. Diabetes Care 2016;39:686–693 - PubMed
-
- Purnell JQ, Zinman B, Brunzell JD; DCCT/EDIC Research Group . The effect of excess weight gain with intensive diabetes mellitus treatment on cardiovascular disease risk factors and atherosclerosis in type 1 diabetes mellitus: results from the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study (DCCT/EDIC) study. Circulation 2013;127:180–187 - PMC - PubMed
-
- Conway B, Miller RG, Costacou T, et al. . Double-edged relationship between adiposity and coronary artery calcification in type 1 diabetes. Diab Vasc Dis Res 2007;4:332–339 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
