

The prevalence of probable neuropathic pain in the US: results from a multimodal general-population health survey
- PMID: 29138590
- PMCID: PMC5677393
- DOI: 10.2147/JPR.S127014
The prevalence of probable neuropathic pain in the US: results from a multimodal general-population health survey
Abstract
Background: The prevalence of neuropathic pain (NeP) has been estimated within specific health conditions; however, there are no published data on its broad prevalence in the US. The current exploratory study addresses this gap using the validated PainDetect questionnaire as a screener for probable NeP in a general-population health survey conducted with a multimodal recruitment strategy to maximize demographic representativeness.
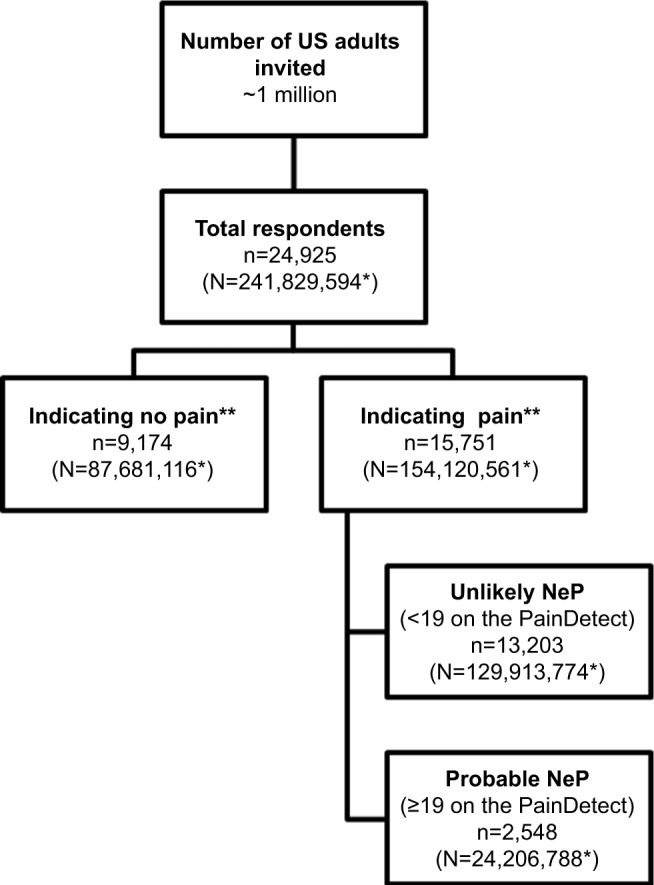
Materials and methods: Adult respondents were recruited from a combination of Internet panels, telephone lists, address lists, mall-based interviews, and store-receipt invitations using a random stratified-sampling framework, with strata defined by age, sex, and race/ethnicity. Older persons and minorities were oversampled to improve prevalence estimates. Results were weighted to match the total adult US population using US Census data. Demographic information was collected, and respondents who experienced physical pain in the past 12 months completed the PainDetect and provided additional pain history. A cutoff score of 19 or greater on the PainDetect was used to define probable NeP.
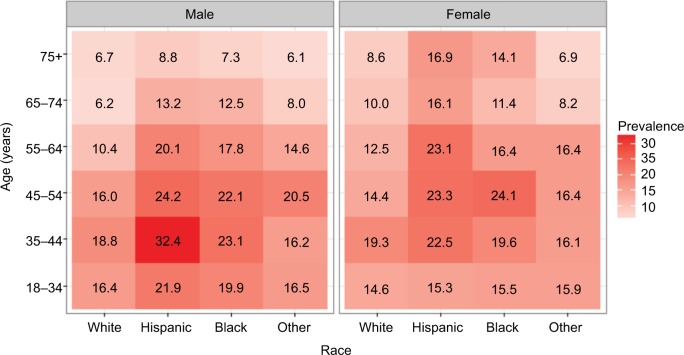
Results: A total of 24,925 respondents (average response rate 2.5%) provided demographic data (52.2% female, mean age 51.5 years); 15,751 respondents reported pain (63.7%), of which 2,548 (15.7%, 95% confidence interval 14.9%-16.5%) had probable NeP based on the PainDetect, which was 10% (95% confidence interval 9.5%-10.5%) of all respondents. Among those reporting pain, the prevalence of probable NeP among Blacks and Hispanics was consistently higher than Whites in each age- and sex group. The highest prevalence among those with pain was among male Hispanics 35-44 years (32.4%) and 45-54 years (24.2%) old. The most commonly used medications reported by those with probable NeP were nonsteroidal anti-inflammatory drugs (44.2%), followed by weak opioids (31.7%), antiepileptics (10.9%), and strong opioids (10.9%).
Conclusion: This is the first study to provide an estimate of the prevalence of probable NeP in the US, showing significant variation by age and ethnicity.
Keywords: epidemiology; neuropathic pain; pain types; prevalence.
Conflict of interest statement
Disclosure AS, MH, BP, JCC, and PH are employees of Pfizer Inc. AHA was employed by Pfizer Inc during and after completion and submission of this study. KC and IK are employees of Kantar Health, which was paid by Pfizer for study design, execution, analysis, and manuscript development. MDD was an employee of Kantar Health at the time of this study. BRS, JDM, and JTF were investigators for the study. They were not financially compensated for their collaborative efforts or publication-related activities, but JTF and JDM have previously served as study design consultant for Pfizer and have received investigator initiated grant funding for studies of pain unrelated to this study. JDM has received research funding from Pfizer for clinical research unrelated to this study. The authors report no other conflicts of interest of this work.
Figures
References
-
- International Association for the Study of Pain Neuropathic pain. 2012. [Accessed January 9, 2017]. Available from: http://www.iasp-pain.org/Education/Content.aspx?ItemNumber=1698&navItemN....
-
- Langley PC, Van Litsenburg C, Cappelleri JC, Carroll D. The burden associated with neuropathic pain in Western Europe. J Med Econ. 2013;16(1):85–95. - PubMed
-
- O’Connor A. Neuropathic pain: quality-of-life impact, costs and cost effectiveness of therapy. Pharmacoeconomics. 2009;27(2):95–112. - PubMed
-
- Bennett MI, Rayment C, Hjermstad M, Aass N, Caraceni A, Kaasa S. Prevalence and aetiology of neuropathic pain in cancer patients: a systematic review. Pain. 2012;153(2):359–365. - PubMed
-
- Argoff CE, Cole BE, Fishbain DA, Irving GA. Diabetic peripheral neuropathic pain: clinical and quality-of-life issues. Mayo Clinic Proceedings. 2006;81(4 Suppl):S3–S11. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
