

Noninvasive Cardiac Testing vs Clinical Evaluation Alone in Acute Chest Pain: A Secondary Analysis of the ROMICAT-II Randomized Clinical Trial
- PMID: 29138794
- PMCID: PMC5838790
- DOI: 10.1001/jamainternmed.2017.7360
Noninvasive Cardiac Testing vs Clinical Evaluation Alone in Acute Chest Pain: A Secondary Analysis of the ROMICAT-II Randomized Clinical Trial
Abstract
Importance: The incremental benefit of noninvasive testing in addition to clinical evaluation (history, physical examination, an electrocardiogram [ECG], and biomarker assessment) vs clinical evaluation alone for patients who present to the emergency department (ED) with acute chest pain is unknown.
Objective: To examine differences in outcomes with clinical evaluation and noninvasive testing (coronary computed tomographic angiography [CCTA] or stress testing) vs clinical evaluation alone.
Design, setting, and participants: This study was a retrospective analysis of data from the randomized multicenter Rule Out Myocardial Ischemia/Infarction by Computer Assisted Tomography (ROMICAT-II) trial. Data for 1000 patients who presented with chest pain to the EDs at 9 hospitals in the United States were evaluated.
Interventions: Clinical evaluation plus noninvasive testing (CCTA or stress test) vs clinical evaluation alone.
Main outcomes and measures: Primary outcome was length of stay (LOS). Secondary outcomes included hospital admission, direct ED discharge, downstream testing, rates of invasive coronary angiography, revascularization, major adverse cardiac events (MACE), repeated ED visit or hospitalization for recurrent chest pain at 28 days, and cost. Safety end points were missed acute coronary syndrome (ACS) and cumulative radiation exposure during the index visit and follow-up period.
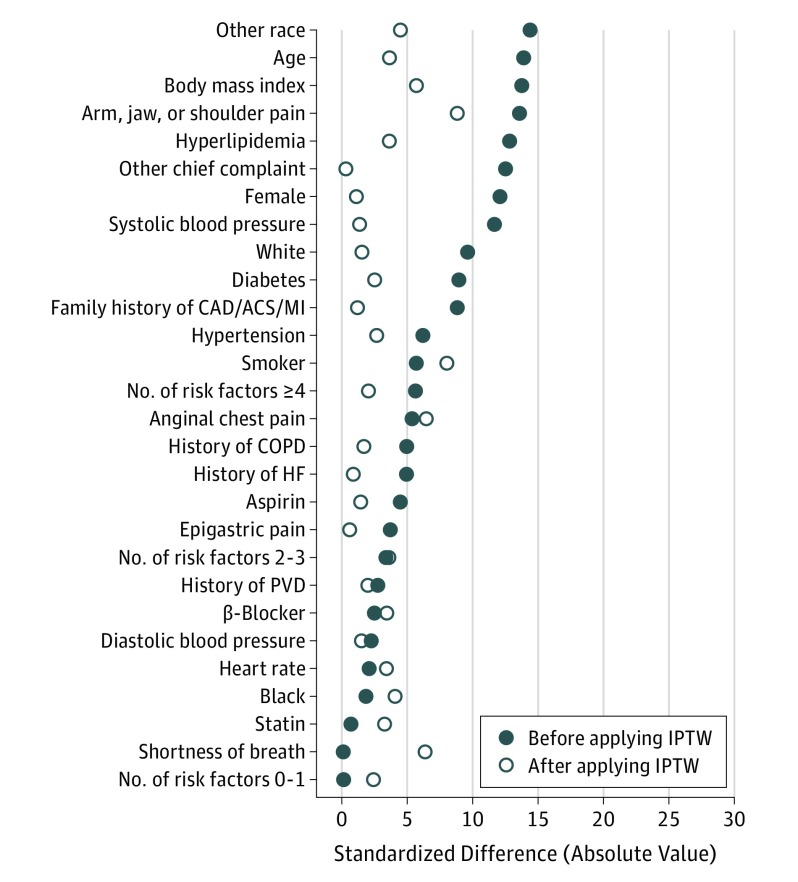
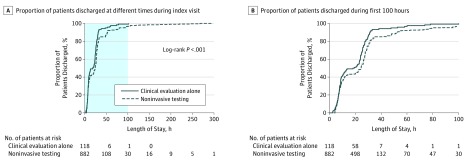
Results: Of the 1000 patients randomized, 118 patients (12%) (mean [SD] age, 53.2 [7.8]; 49 [42%] were female) did not undergo noninvasive testing, whereas 882 (88%) (mean [SD] age, 54.4 [8.14] years; 419 [48%] were female) received CCTA or stress testing. There was no difference in baseline characteristics or clinical presentation between groups. Patients who underwent clinical evaluation alone experienced a shorter LOS (20.3 vs 27.9 hours; P < .001), lower rates of diagnostic testing (P < .001) and angiography (2% vs 11%; P < .001), lower median costs ($2261.50 vs $2584.30; P = .009), and less cumulative radiation exposure (0 vs 9.9 mSv; P < .001) during the 28-day study period. Lack of testing was associated with a lower rate of diagnosis of ACS (0% vs 9%; P < .001) and less coronary angiography and percutaneous coronary intervention (PCI) during the index visit (0% vs 10%; P < .001, and 0% vs 4%; P = .02, respectively). There was no difference in rates of PCI (2% vs 5%; P = .15), coronary artery bypass surgery (0% vs 1%; P = .61), return ED visits (5.8% vs 2.8%; P = .08), or MACE (2% vs 1%; P = .24) in the 28-day follow-up period.
Conclusions and relevance: In patients presenting to the ED with acute chest pain, negative biomarkers, and a nonischemic ECG result, noninvasive testing with CCTA or stress testing leads to longer LOS, more downstream testing, more radiation exposure, and greater cost without an improvement in clinical outcomes.
Trial registration: clinicaltrials.gov Identifier: NCT01084239.
Conflict of interest statement
Figures
Comment in
-
Acute Chest Pain in the Emergency Department.JAMA Intern Med. 2018 Feb 1;178(2):220. doi: 10.1001/jamainternmed.2017.7519. JAMA Intern Med. 2018. PMID: 29138793 No abstract available.
-
Incorrect Conclusions of a Secondary Analysis.JAMA Intern Med. 2018 Apr 1;178(4):581-582. doi: 10.1001/jamainternmed.2018.0212. JAMA Intern Med. 2018. PMID: 29610879 No abstract available.
-
Incorrect Conclusions of a Secondary Analysis-Reply.JAMA Intern Med. 2018 Apr 1;178(4):582. doi: 10.1001/jamainternmed.2018.0187. JAMA Intern Med. 2018. PMID: 29610891 No abstract available.
-
Incorrect Conclusions of a Secondary Analysis-Reply.JAMA Intern Med. 2018 Apr 1;178(4):582-583. doi: 10.1001/jamainternmed.2018.0203. JAMA Intern Med. 2018. PMID: 29610892 No abstract available.
References
-
- Anderson JL, Adams CD, Antman EM, et al. ; American College of Cardiology; American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction); American College of Emergency Physicians; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons; American Association of Cardiovascular and Pulmonary Rehabilitation; Society for Academic Emergency Medicine . ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50(7):e1-e157. - PubMed
-
- Owens PL, Barrett ML, Gibson TB, Andrews RM, Weinick RM, Mutter RL. Emergency department care in the United States: a profile of national data sources. Ann Emerg Med. 2010;56(2):150-165. - PubMed
-
- Pope JH, Aufderheide TP, Ruthazer R, et al. . Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med. 2000;342(16):1163-1170. - PubMed
-
- Kline JA, Jones AE, Shapiro NI, et al. . Multicenter, randomized trial of quantitative pretest probability to reduce unnecessary medical radiation exposure in emergency department patients with chest pain and dyspnea. Circ Cardiovasc Imaging. 2014;7(1):66-73. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
