

Vessel centerline reconstruction from non-isocentric and non-orthogonal paired monoplane angiographic images
- PMID: 29139034
- PMCID: PMC5889725
- DOI: 10.1007/s10554-017-1275-z
Vessel centerline reconstruction from non-isocentric and non-orthogonal paired monoplane angiographic images
Abstract
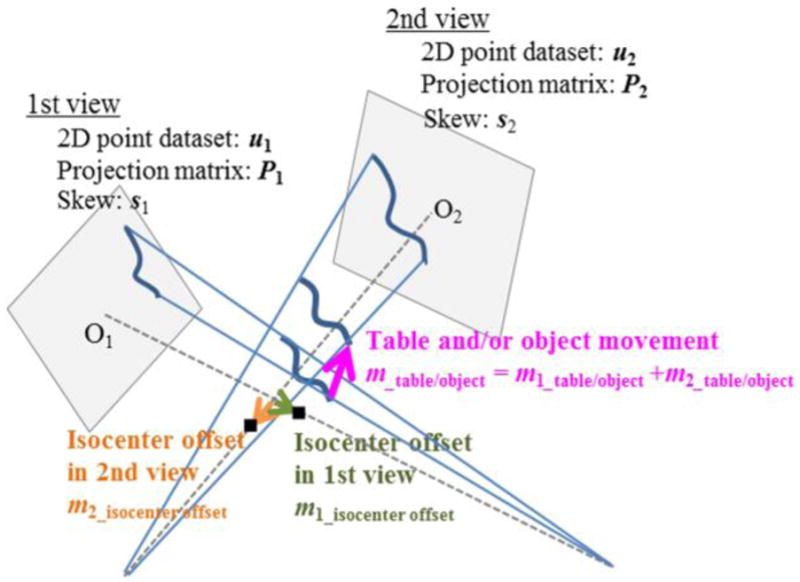
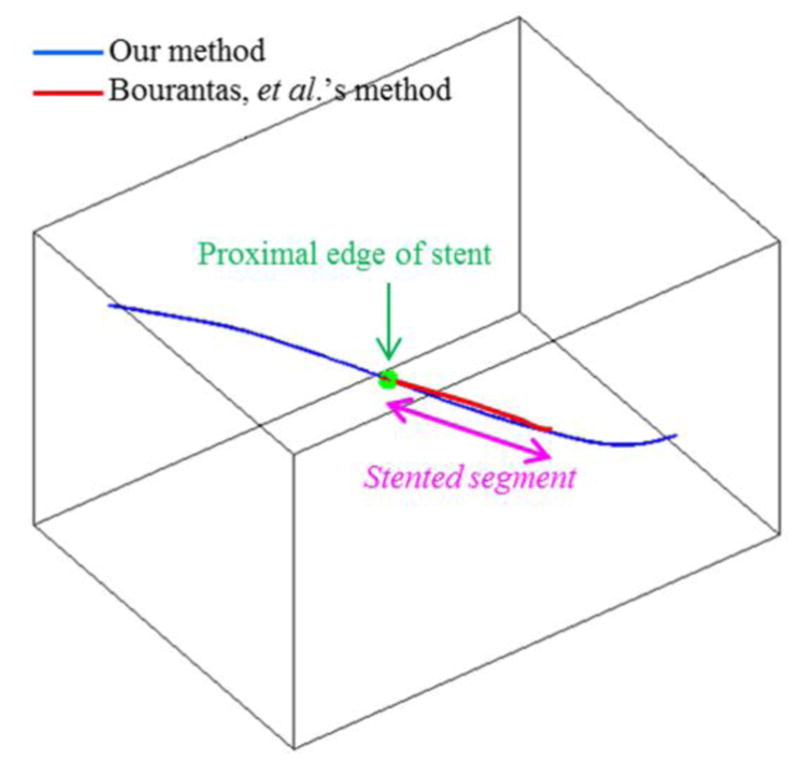
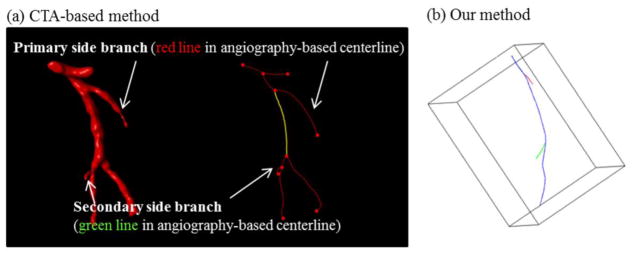
Purpose: Three-dimensional reconstruction of a vessel centerline from paired planar coronary angiographic images is critical to reconstruct the complex three-dimensional structure of the coronary artery lumen and the relative positioning of implanted devices. In this study, a new vessel centerline reconstruction method that can utilize non-isocentric and non-orthogonal pairs of angiographic images was developed and tested.
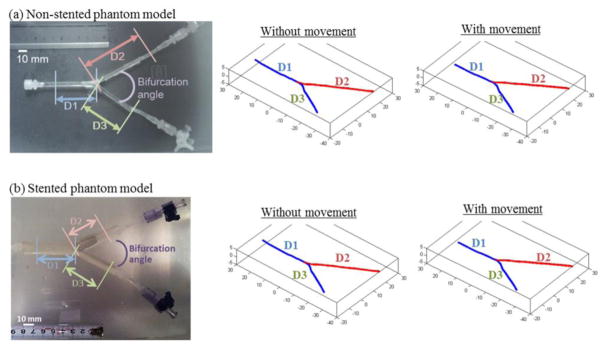
Methods: Our new method was developed in in vitro phantom models of bifurcated coronary artery with and without stent, and then tested in in vivo swine models (twelve coronary arteries). This method was also validated using data from six patients.
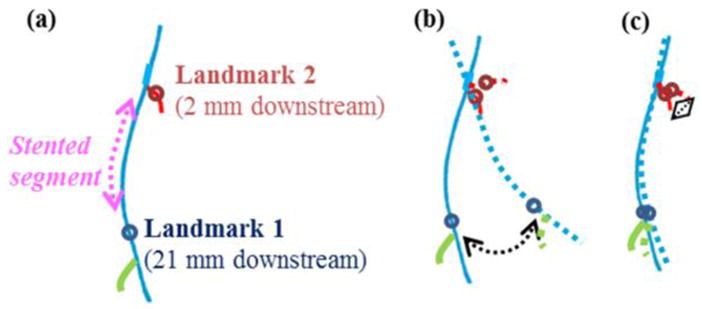
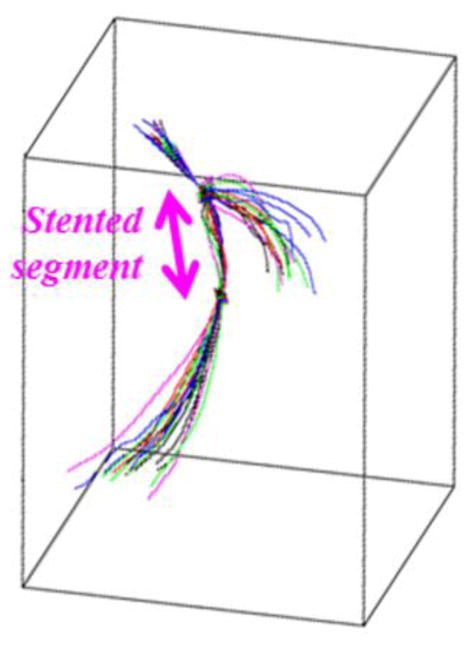
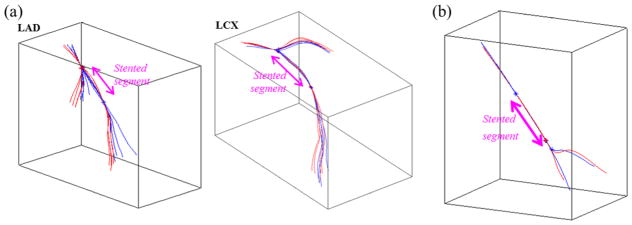
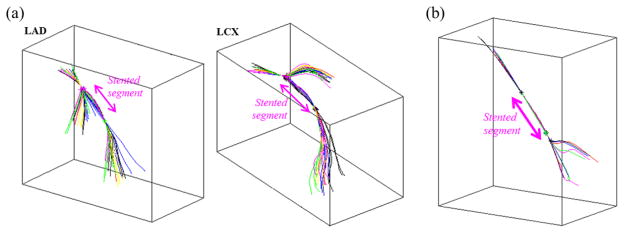
Results: Our new method demonstrated high accuracy (root mean square error = 0.27 mm or 0.76 pixel), and high reproducibility across a broad imaging angle (20°-130°) and between different cardiac cycles in vitro and in vivo. Use of this method demonstrated that the vessel centerline in the stented segment did not deform significantly over a cardiac cycle in vivo. In addition, the total movement of the isocenter in each image could be accurately estimated in vitro and in vivo. The performance of this new method for patient data was similar to that for in vitro phantom models and in vivo animal models.
Conclusions: We developed a vessel centerline reconstruction method for non-isocentric and non-orthogonal angiographic images. It demonstrated high accuracy and good reproducibility in vitro, in vivo, and in clinical setting, suggesting that our new method is clinically applicable despite the small sample size of clinical data.
Keywords: Coronary angiography; Image reconstruction; Reconstruction algorithm; Stereoscopic theory.
Figures
References
-
- Thompson CA. Textbook of Cardiovascular Intervention. 1. Springer; 2014. - DOI
-
- Dowe DA, Fioranelli M, Pavone P. Imaging Croronary Arteries. 2. Springer; 2013.
-
- Chen SY, Carroll Jd, Messenger JC, Messenger JC. Quantitative analysis of reconstructed 3-D coronary arterial tree and intracoronary devices. IEEE Trans Med Imaging. 2002;21(7):724–749. - PubMed
-
- Dvir D, Marom H, Guetta V, Kornowski R. Three-dimensional coronary reconstruction from routine single-plane coronary angiograms: in vivo quantitative validation. Int J Cardiovasc Intervent. 2005;7:141–145. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
