

Local alkylating chemotherapy applied immediately after 5-ALA guided resection of glioblastoma does not provide additional benefit
- PMID: 29139095
- PMCID: PMC5770495
- DOI: 10.1007/s11060-017-2649-8
Local alkylating chemotherapy applied immediately after 5-ALA guided resection of glioblastoma does not provide additional benefit
Abstract
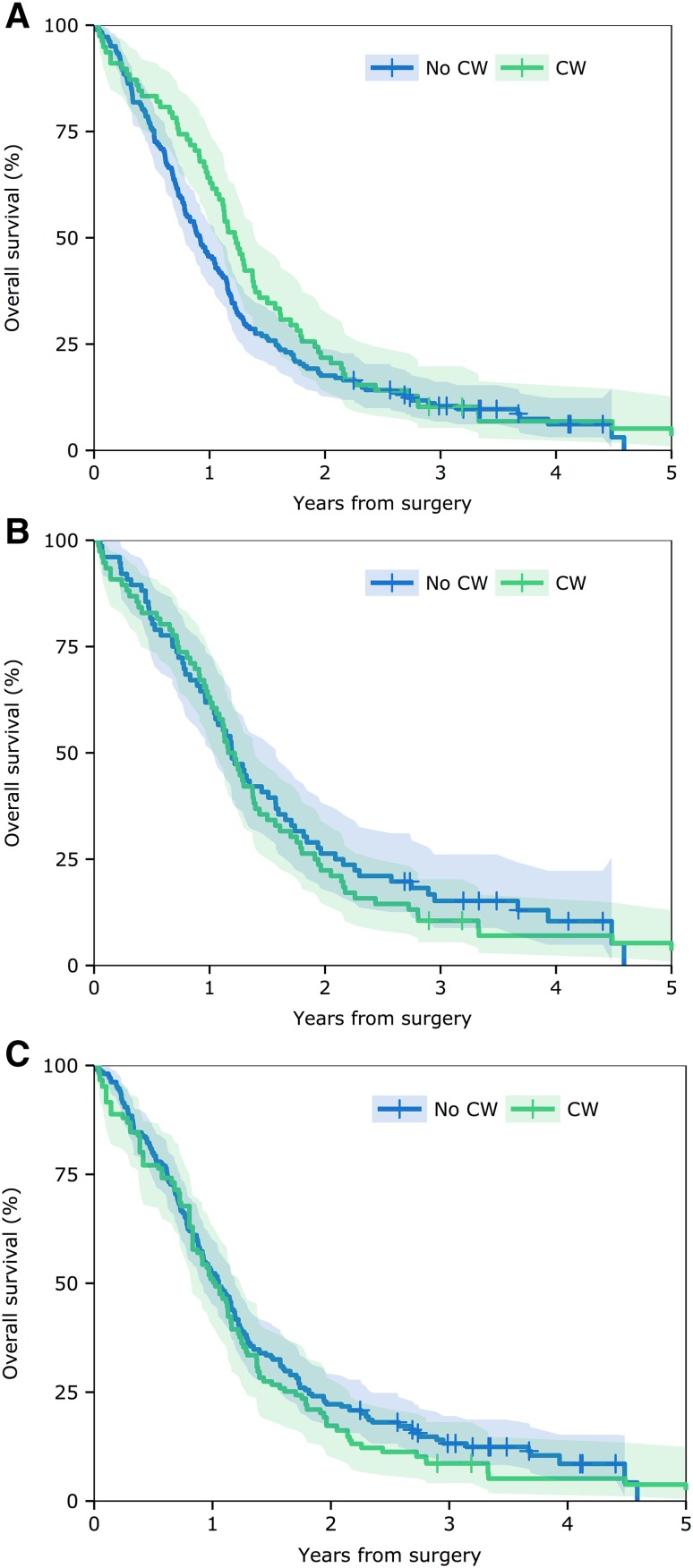
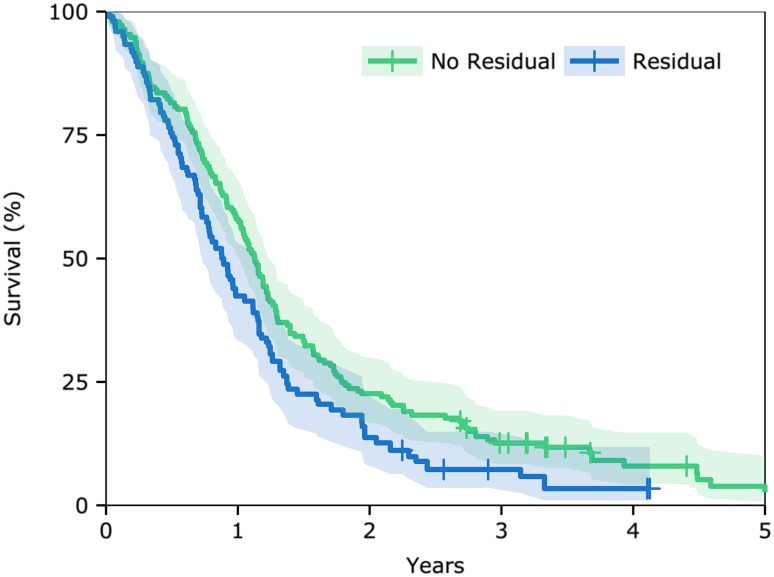
Grade IV glioma is the most common and aggressive primary brain tumour. Gross total resection with 5-aminolevulinic acid (5-ALA) guided surgery combined with local chemotherapy (carmustine wafers) is an attractive treatment strategy in these patients. No previous studies have examined the benefit carmustine wafers in a treatment programme of 5-ALA guided resection followed by a temozolomide-based chemoradiotherapy protocol. The objective of this study was to examine the benefit of carmustine wafers on survival in patients undergoing 5-ALA guided resection. A retrospective cohort study of 260 patients who underwent 5-ALA resection of confirmed WHO 2007 Grade IV glioma between July 2009 and December 2014. Survival curves were calculated using the Kaplan-Meier method from surgery. The log-rank test was used to compare survival curves between groups. Cox regression was performed to identify variables predicting survival. A propensity score matched analysis was used to compare survival between patients who did and did not receive carmustine wafers while controlling for baseline characteristics. Propensity matched analysis showed no significant survival benefit of insertion of carmustine wafers over 5-ALA resection alone (HR 0.97 [0.68-1.26], p = 0.836). There was a trend to higher incidence of wound infection in those who received carmustine wafers (15.4 vs. 7.1%, p = 0.064). The Cox regression analysis showed that intraoperative residual fluorescent tumour and residual enhancing tumour on post-operative MRI were significantly predictive of reduced survival. Carmustine wafers have no added benefit following 5-ALA guided resection. Residual fluorescence and residual enhancing disease following resection have a negative impact on survival.
Keywords: 5-Aminolevulinic acid; Carmustine; Glioma; Neurosurgery.
Conflict of interest statement
No conflict of interest declared.
Figures
Comment in
-
Letter to the editor: local alkylating chemotherapy applied immediately after 5-ALA guided resection of glioblastoma does not provide additional benefit.J Neurooncol. 2018 May;138(1):217-218. doi: 10.1007/s11060-018-2770-3. Epub 2018 Jan 20. J Neurooncol. 2018. PMID: 29353435 No abstract available.
References
-
- Stummer W, Meinel T, Ewelt C, et al. Prospective cohort study of radiotherapy with concominant and adjuvant temozolomide chemotherapy for glioblastoma patients with no or minimal residual enhancing tumor load after surgery. J Neurooncol. 2012;108(1):89–97. doi: 10.1007/s11060-012-0798-3. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
