

Lymphangioleiomyomatosis Diagnosis and Management: High-Resolution Chest Computed Tomography, Transbronchial Lung Biopsy, and Pleural Disease Management. An Official American Thoracic Society/Japanese Respiratory Society Clinical Practice Guideline
- PMID: 29140122
- PMCID: PMC5694834
- DOI: 10.1164/rccm.201709-1965ST
Lymphangioleiomyomatosis Diagnosis and Management: High-Resolution Chest Computed Tomography, Transbronchial Lung Biopsy, and Pleural Disease Management. An Official American Thoracic Society/Japanese Respiratory Society Clinical Practice Guideline
Abstract
Background: Recommendations regarding key aspects related to the diagnosis and pharmacological treatment of lymphangioleiomyomatosis (LAM) were recently published. We now provide additional recommendations regarding four specific questions related to the diagnosis of LAM and management of pneumothoraces in patients with LAM.
Methods: Systematic reviews were performed and then discussed by a multidisciplinary panel. For each intervention, the panel considered its confidence in the estimated effects, the balance of desirable (i.e., benefits) and undesirable (i.e., harms and burdens) consequences, patient values and preferences, cost, and feasibility. Evidence-based recommendations were then formulated, written, and graded using the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) approach.
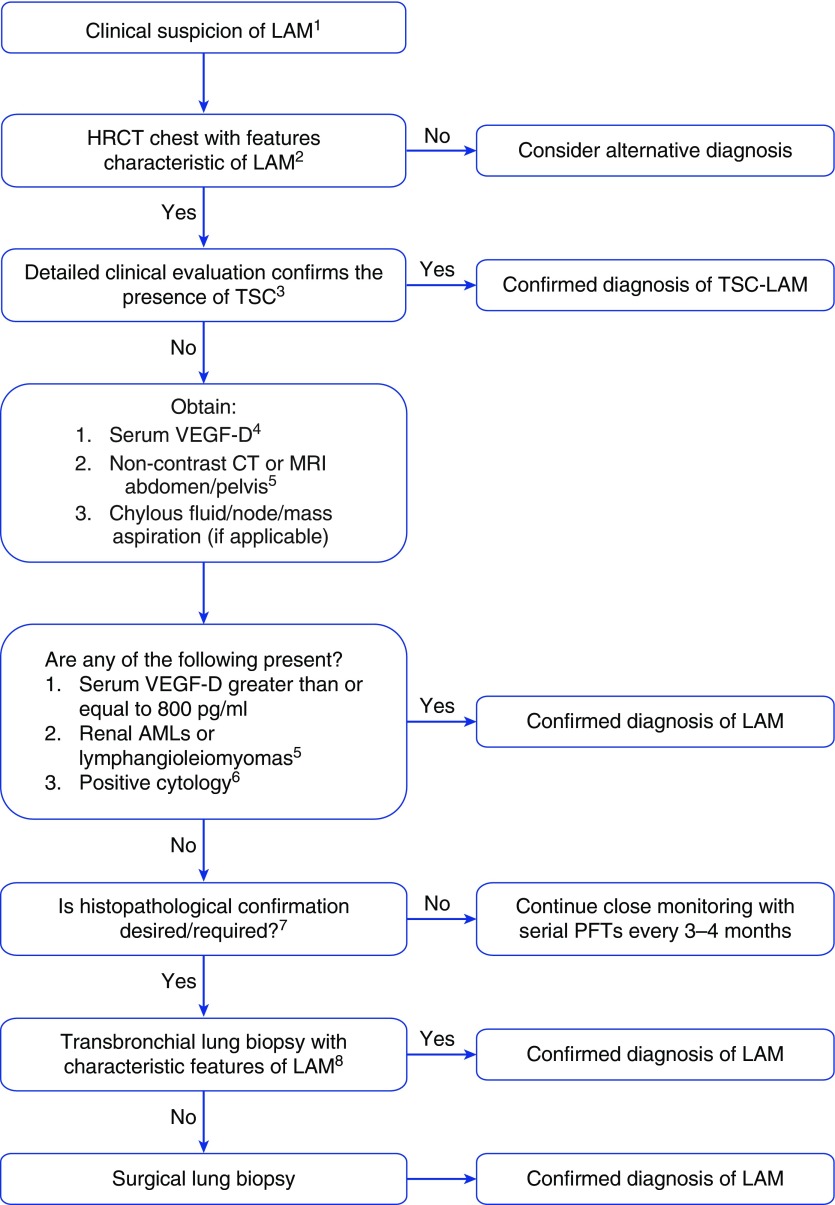
Results: For women who have cystic changes on high-resolution computed tomography of the chest characteristic of LAM, but who have no additional confirmatory features of LAM (i.e., clinical, radiologic, or serologic), the guideline panel made conditional recommendations against making a clinical diagnosis of LAM on the basis of the high-resolution computed tomography findings alone and for considering transbronchial lung biopsy as a diagnostic tool. The guideline panel also made conditional recommendations for offering pleurodesis after an initial pneumothorax rather than postponing the procedure until the first recurrence and against pleurodesis being used as a reason to exclude patients from lung transplantation.
Conclusions: Evidence-based recommendations for the diagnosis and treatment of patients with LAM are provided. Frequent reassessment and updating will be needed.
Figures
Comment in
-
Treatment of Pulmonary Lymphangioleiomyomatosis during Pregnancy.Am J Respir Crit Care Med. 2018 Jun 1;197(11):1506-1507. doi: 10.1164/rccm.201712-2566LE. Am J Respir Crit Care Med. 2018. PMID: 29356556 No abstract available.
-
Reply to Yanagisawa: Treatment of Pulmonary Lymphangioleiomyomatosis during Pregnancy.Am J Respir Crit Care Med. 2018 Jun 1;197(11):1507-1508. doi: 10.1164/rccm.201801-0043LE. Am J Respir Crit Care Med. 2018. PMID: 29356560 Free PMC article. No abstract available.
References
-
- McCormack FX, Gupta N, Finlay GR, Young LR, Taveira-DaSilva AM, Glasgow CG, Steagall WK, Johnson SR, Sahn SA, Ryu JH, et al. ATS/JRS Committee on Lymphangioleiomyomatosis. Official American Thoracic Society/Japanese Respiratory society clinical practice guidelines: lymphangioleiomyomatosis diagnosis and management. Am J Respir Crit Care Med. 2016;194:748–761. - PMC - PubMed
-
- Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, Norris S, Falck-Ytter Y, Glasziou P, DeBeer H, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64:383–394. - PubMed
-
- Guyatt GH, Oxman AD, Kunz R, Atkins D, Brozek J, Vist G, Alderson P, Glasziou P, Falck-Ytter Y, Schünemann HJ. GRADE guidelines: 2. Framing the question and deciding on important outcomes. J Clin Epidemiol. 2011;64:395–400. - PubMed
-
- Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J, Vist GE, Falck-Ytter Y, Meerpohl J, Norris S, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64:401–406. - PubMed
-
- Johnson SR, Cordier JF, Lazor R, Cottin V, Costabel U, Harari S, Reynaud-Gaubert M, Boehler A, Brauner M, Popper H, et al. Review Panel of the ERS LAM Task Force. European Respiratory Society guidelines for the diagnosis and management of lymphangioleiomyomatosis. Eur Respir J. 2010;35:14–26. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
