

Effectiveness of Masks and Respirators Against Respiratory Infections in Healthcare Workers: A Systematic Review and Meta-Analysis
- PMID: 29140516
- PMCID: PMC7108111
- DOI: 10.1093/cid/cix681
Effectiveness of Masks and Respirators Against Respiratory Infections in Healthcare Workers: A Systematic Review and Meta-Analysis
Abstract
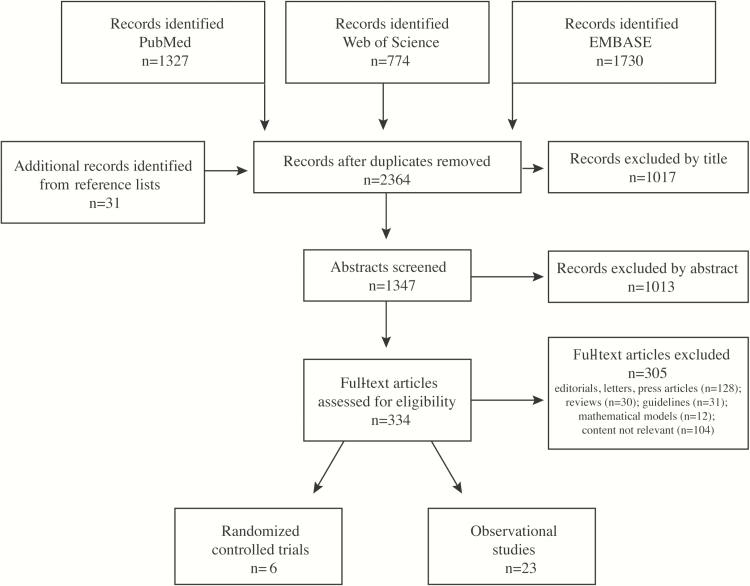
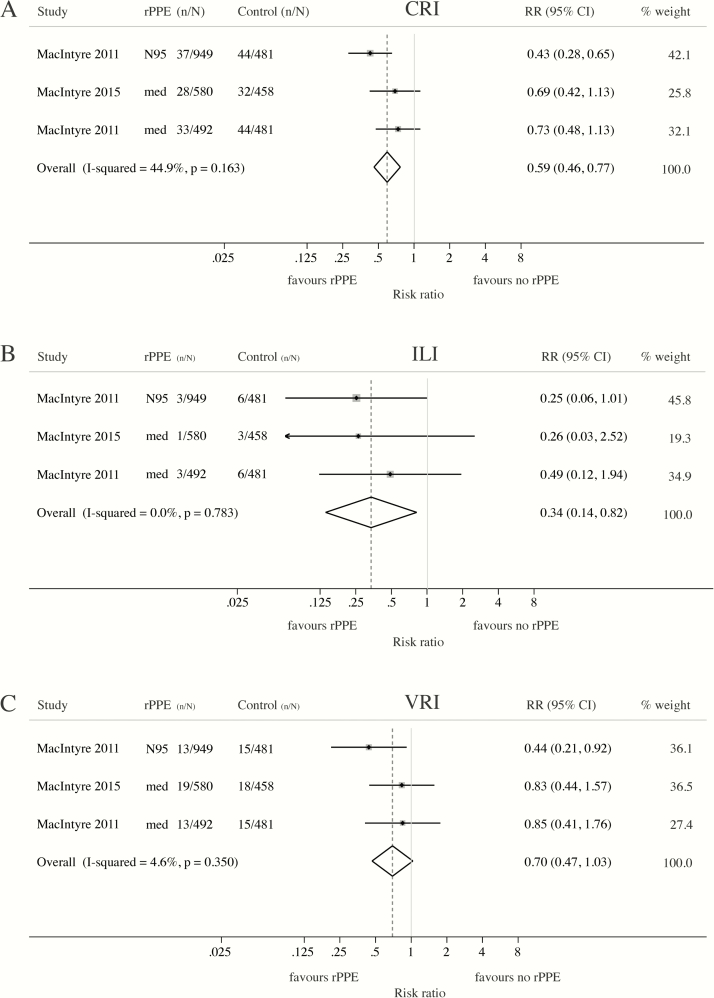
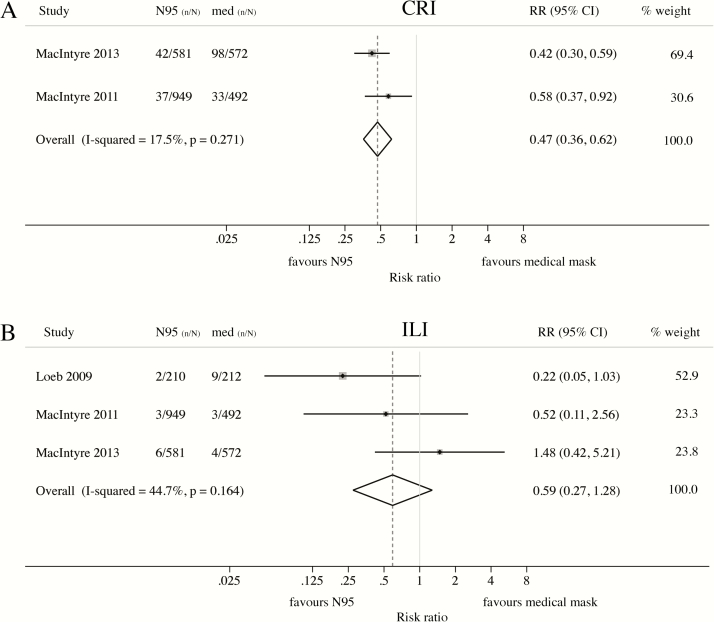
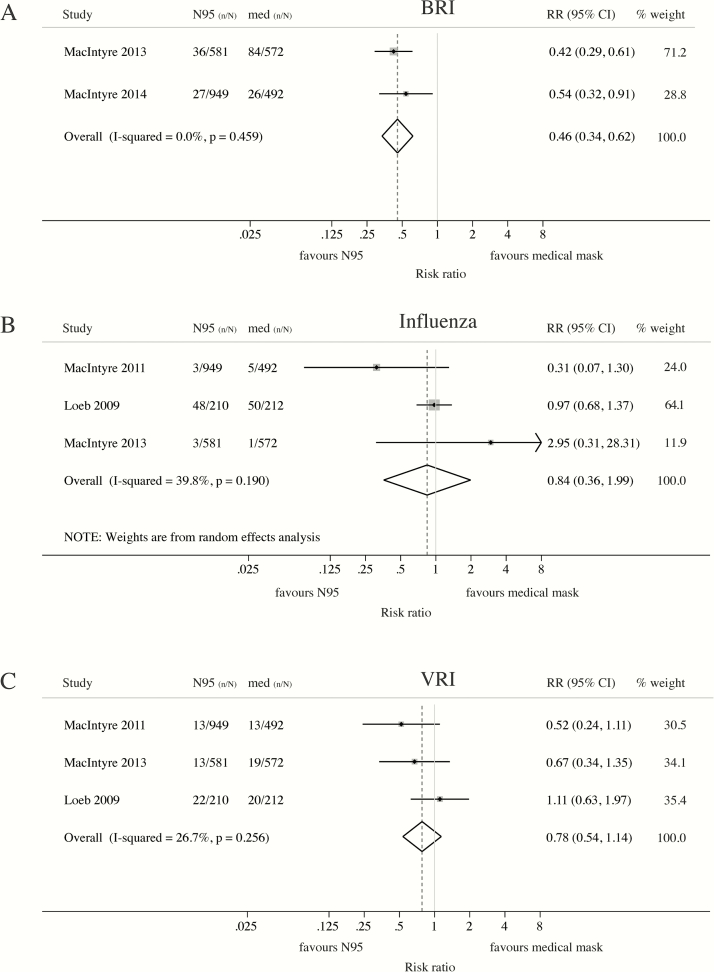
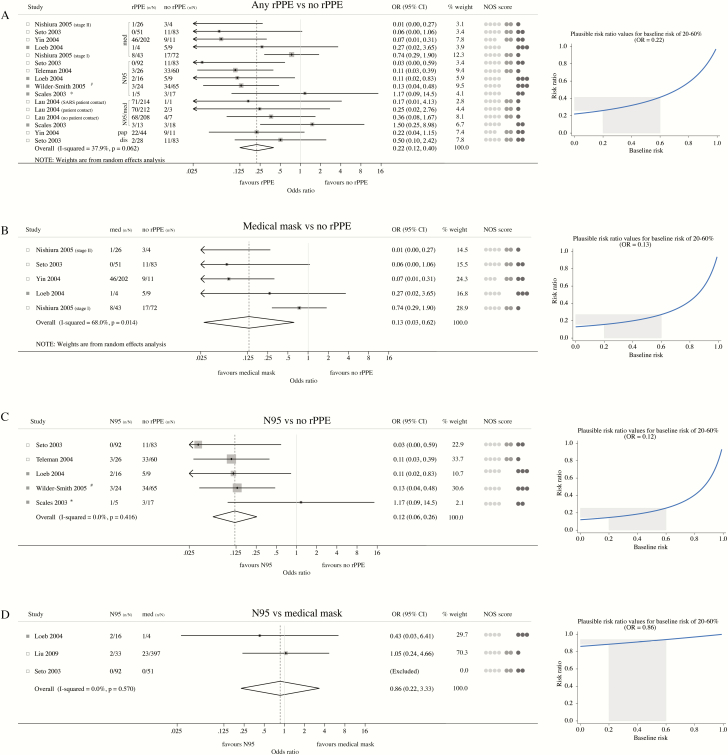
This systematic review and meta-analysis quantified the protective effect of facemasks and respirators against respiratory infections among healthcare workers. Relevant articles were retrieved from Pubmed, EMBASE, and Web of Science. Meta-analyses were conducted to calculate pooled estimates. Meta-analysis of randomized controlled trials (RCTs) indicated a protective effect of masks and respirators against clinical respiratory illness (CRI) (risk ratio [RR] = 0.59; 95% confidence interval [CI]:0.46-0.77) and influenza-like illness (ILI) (RR = 0.34; 95% CI:0.14-0.82). Compared to masks, N95 respirators conferred superior protection against CRI (RR = 0.47; 95% CI: 0.36-0.62) and laboratory-confirmed bacterial (RR = 0.46; 95% CI: 0.34-0.62), but not viral infections or ILI. Meta-analysis of observational studies provided evidence of a protective effect of masks (OR = 0.13; 95% CI: 0.03-0.62) and respirators (OR = 0.12; 95% CI: 0.06-0.26) against severe acute respiratory syndrome (SARS). This systematic review and meta-analysis supports the use of respiratory protection. However, the existing evidence is sparse and findings are inconsistent within and across studies. Multicentre RCTs with standardized protocols conducted outside epidemic periods would help to clarify the circumstances under which the use of masks or respirators is most warranted.
Keywords: Facemasks; N95 respirators; influenza; respiratory infections; severe acute respiratory syndrome (SARS).
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Peiris JS, Tu WW, Yen HL. A novel H1N1 virus causes the first pandemic of the 21st century. Eur J Immunol 2009; 39:2946–54. - PubMed
-
- Trajman A, Menzies D. Occupational respiratory infections. Curr Opin Pulm Med 2010; 16:226–34. - PubMed
-
- World Health Organization. Infection prevention and control of epidemic- and pandemic-prone acute respiratory infections in health care Geneva, Switzerland: 2014; Available at: http://apps.who.int/iris/bitstream/10665/112656/1/9789241507134_eng.pdf. Accessed 27 April 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
