

Medical therapy versus radiofrequency endometrial ablation in the initial treatment of heavy menstrual bleeding (iTOM Trial): A clinical and economic analysis
- PMID: 29141040
- PMCID: PMC5687740
- DOI: 10.1371/journal.pone.0188176
Medical therapy versus radiofrequency endometrial ablation in the initial treatment of heavy menstrual bleeding (iTOM Trial): A clinical and economic analysis
Abstract
Background: Radiofrequency endometrial ablation (REA) is currently a second line treatment in women with heavy menstrual bleeding (MHB) if medical therapy (MTP) is contraindicated or unsatisfactory. Our objective is to compare the effectiveness and cost burden of MTP and REA in the initial treatment of HMB.
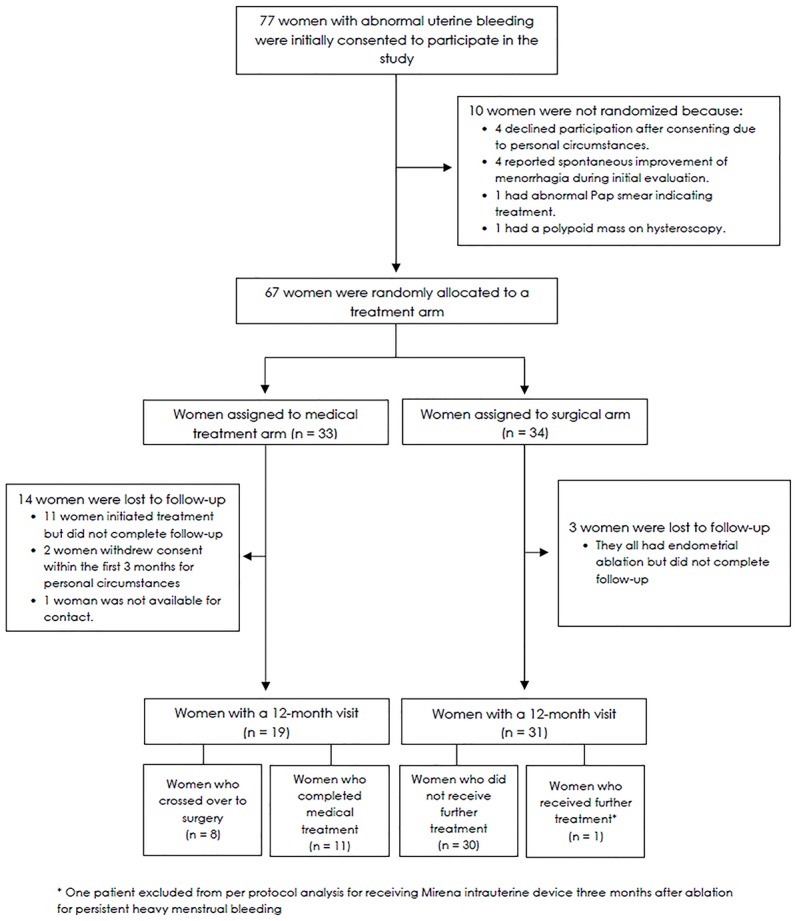
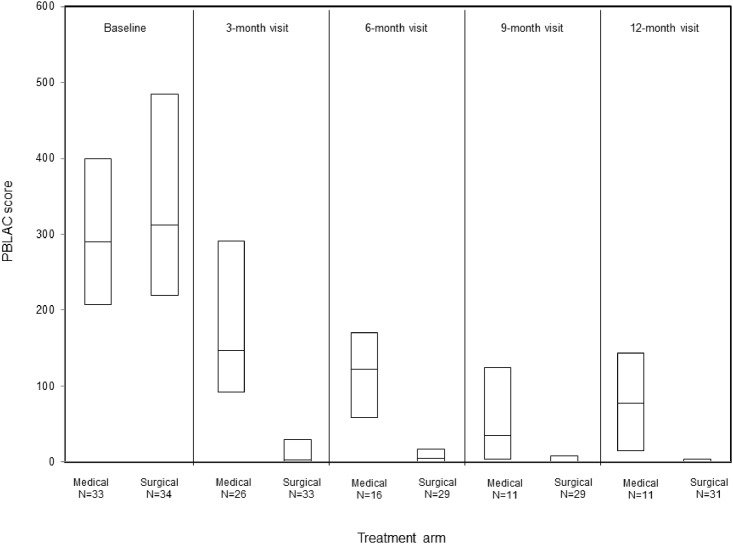
Methods: We performed a randomized trial at Mayo Clinic Rochester, Minnesota. The planned sample size was 60 patients per arm. A total of 67 women with HMB were randomly allocated to receive oral contraceptive pills (Nordette ®) or Naproxen (Naprosyn®) (n = 33) or REA (n = 34). Primary 12-month outcome measures included menstrual blood loss using pictorial blood loss assessment chart (PBLAC), patients' satisfaction, and Menorrhagia Multi-Attribute Scale (MMAS). Secondary outcomes were total costs including direct medical and indirect costs associated with healthcare use, patient out-of-pocket costs, and lost work days and activity limitations over 12 months.
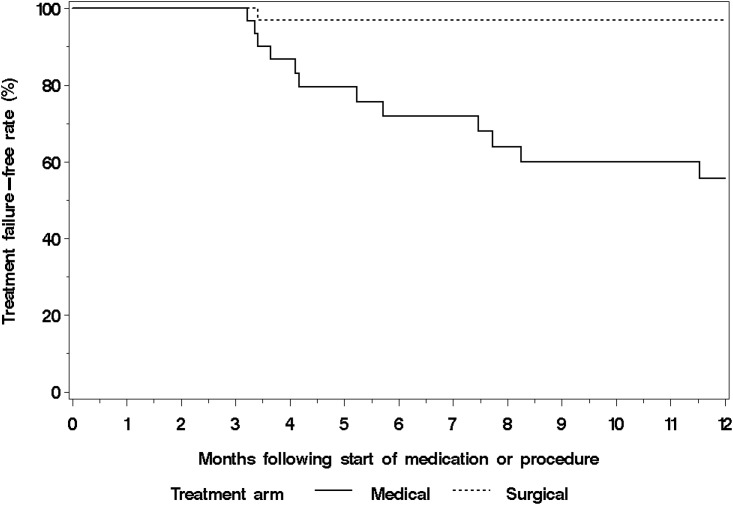
Results: Compared to MTP arm, women who received REA had a significantly lower PBLAC score (median [Interquartile range, IQR]: 0 [0-4] vs. 15 [0-131], p = 0.003), higher satisfaction rates (96.8%vs.63.2%, p = 0.003) and higher MMAS (median [IQR]: 100 [100-100] vs. 100 [87-100], p = 0.12) at 12 months. Direct medical costs were higher for REA ($5,331vs.$2,901, 95% confidence interval (CI) of mean difference:$727,$4,852), however, when indirect costs are included, the difference did not reach statistical significance ($5,469 vs. $3,869, 95% CI of mean difference:-$339, $4,089).
Conclusion: For women with heavy menstrual bleeding, initial radiofrequency endometrial ablation compared to medical therapy offered superior reduction in menstrual blood loss and improvement in quality of life without significant differences in total costs of care.
Clinical trial registration: NCT01165307.
Conflict of interest statement
Figures
References
-
- Côté I, Jacobs P, Cumming D. Work loss associated with increased menstrual loss in the United States. Obstetrics & Gynecology. 2002;100(4):683–7. - PubMed
-
- Côté I, Jacobs P, Cumming DC. Use of health services associated with increased menstrual loss in the United States. American journal of obstetrics and gynecology. 2003;188(2):343–8. - PubMed
-
- American College of Obstetricians and Gynecologists. Endometrial ablation: ACOG practice bulletin no. 81. Obstet Gynecol. 2007;109:1233–48. - PubMed
-
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 110: noncontraceptive uses of hormonal contraceptives. Obstet Gynecol. 2010;115(1):206–18. - PubMed
-
- Cravello L, Agostini A, Beerli M, Roger V, Bretelle F, Blanc B. [Results of hysteroscopic myomectomy]. Gynecologie, obstetrique & fertilite. 2004;32(9):825–8. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
