

Using Observational Data to Calibrate Simulation Models
- PMID: 29141153
- PMCID: PMC5771959
- DOI: 10.1177/0272989X17738753
Using Observational Data to Calibrate Simulation Models
Abstract
Background: Individual-level simulation models are valuable tools for comparing the impact of clinical or public health interventions on population health and cost outcomes over time. However, a key challenge is ensuring that outcome estimates correctly reflect real-world impacts. Calibration to targets obtained from randomized trials may be insufficient if trials do not exist for populations, time periods, or interventions of interest. Observational data can provide a wider range of calibration targets but requires methods to adjust for treatment-confounder feedback. We propose the use of the parametric g-formula to estimate calibration targets and present a case-study to demonstrate its application.
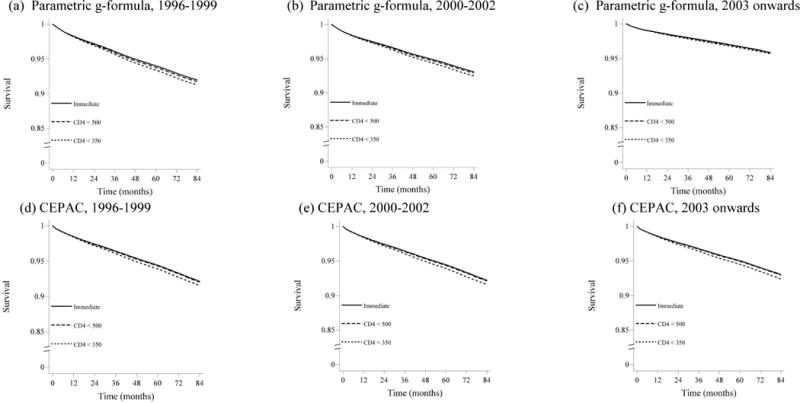
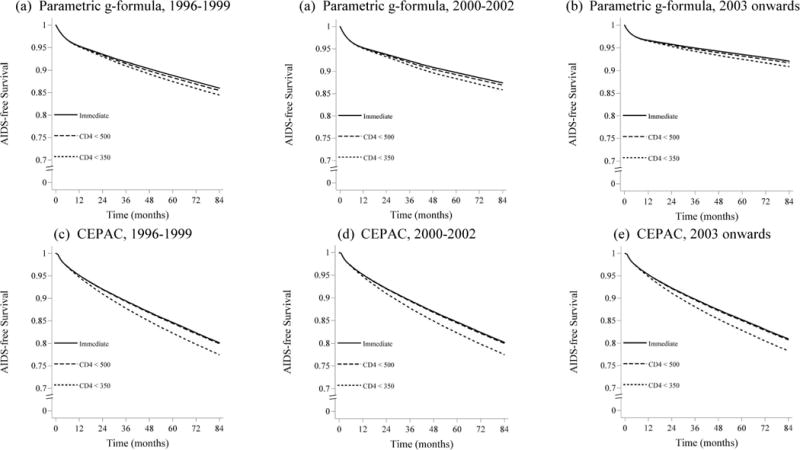
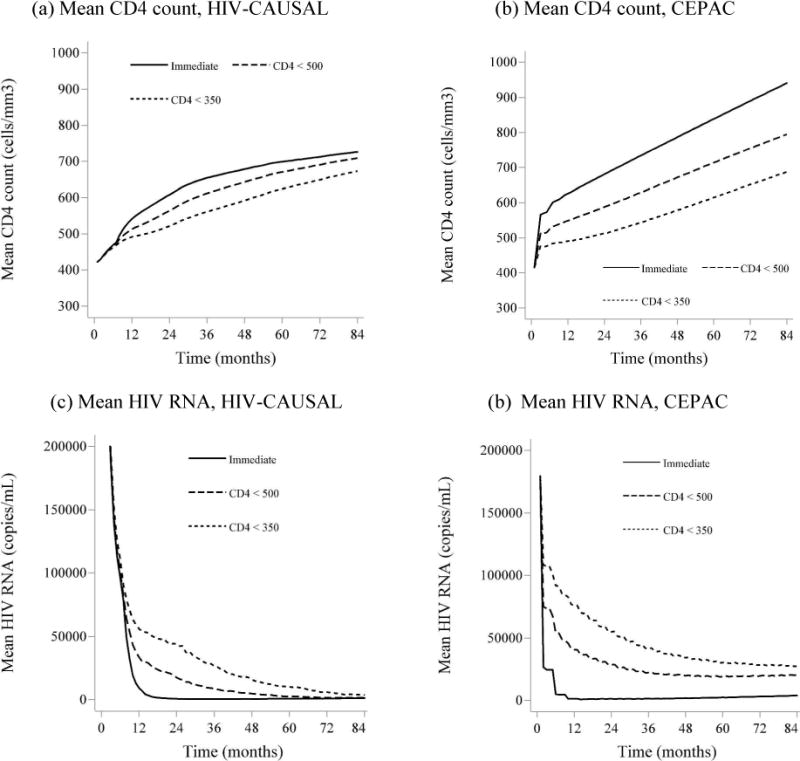
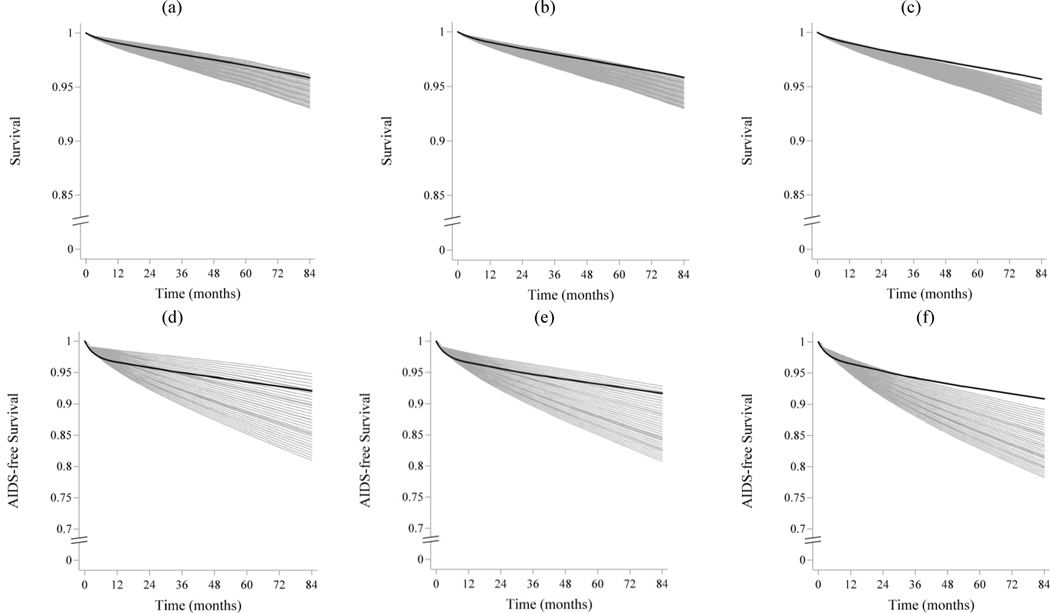
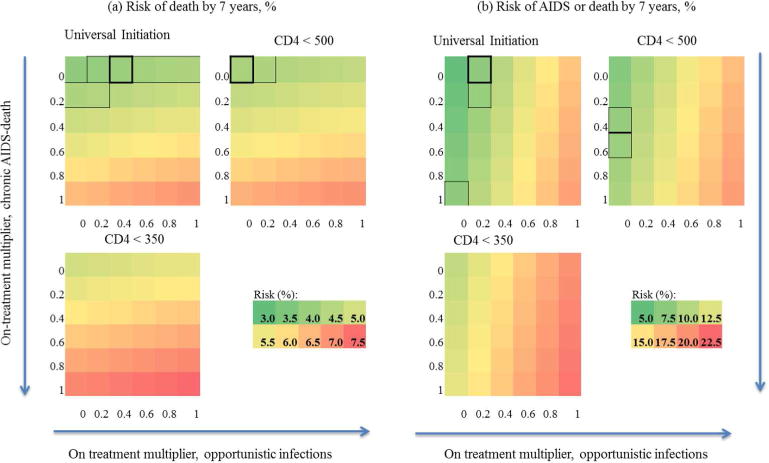
Methods: We used the parametric g-formula applied to data from the HIV-CAUSAL Collaboration to estimate calibration targets for 7-y risks of AIDS and/or death (AIDS/death), as defined by the Center for Disease Control and Prevention under 3 treatment initiation strategies. We compared these targets to projections from the Cost-effectiveness of Preventing AIDS Complications (CEPAC) model for treatment-naïve individuals presenting to care in the following year ranges: 1996 to 1999, 2000 to 2002, or 2003 onwards.
Results: The parametric g-formula estimated a decreased risk of AIDS/death over time and with earlier treatment. The uncalibrated CEPAC model successfully reproduced targets obtained via the g-formula for baseline 1996 to 1999, but over-estimated calibration targets in contemporary populations and failed to reproduce time trends in AIDS/death risk. Calibration to g-formula targets improved CEPAC model fit for contemporary populations.
Conclusion: Individual-level simulation models are developed based on best available information about disease processes in one or more populations of interest, but these processes can change over time or between populations. The parametric g-formula provides a method for using observational data to obtain valid calibration targets and enables updating of simulation model inputs when randomized trials are not available.
Keywords: HIV; agent-based model; calibration; g-formula.
Figures

References
-
- Weinstein MC, O’Brien B, Hornberger J, Jackson J, Johannesson M, McCabe C, et al. Principles of good practice for decision analytic modeling in health-care evaluation: report of the ISPOR task force on good research practices–modeling studies. Value in Health. 2003;6(1):9–17. Epub 2003/01/22. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
