

A Comprehensive Patient-Derived Xenograft Collection Representing the Heterogeneity of Melanoma
- PMID: 29141225
- PMCID: PMC5726788
- DOI: 10.1016/j.celrep.2017.10.021
A Comprehensive Patient-Derived Xenograft Collection Representing the Heterogeneity of Melanoma
Abstract
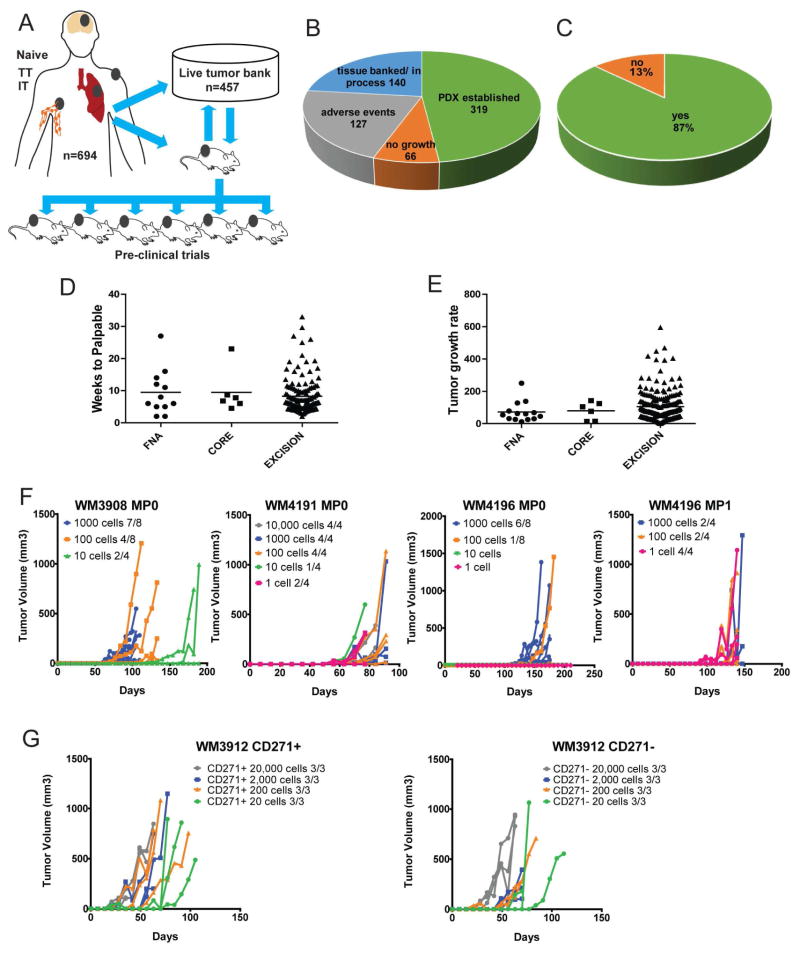
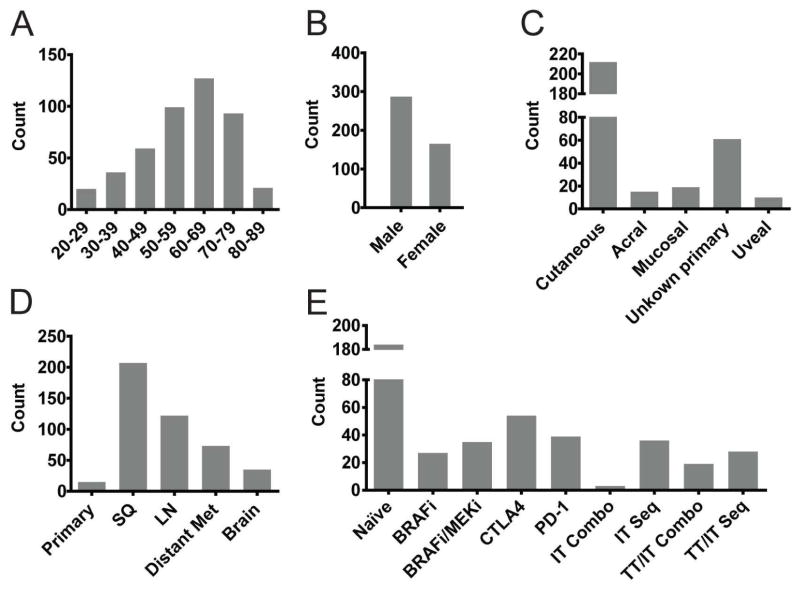
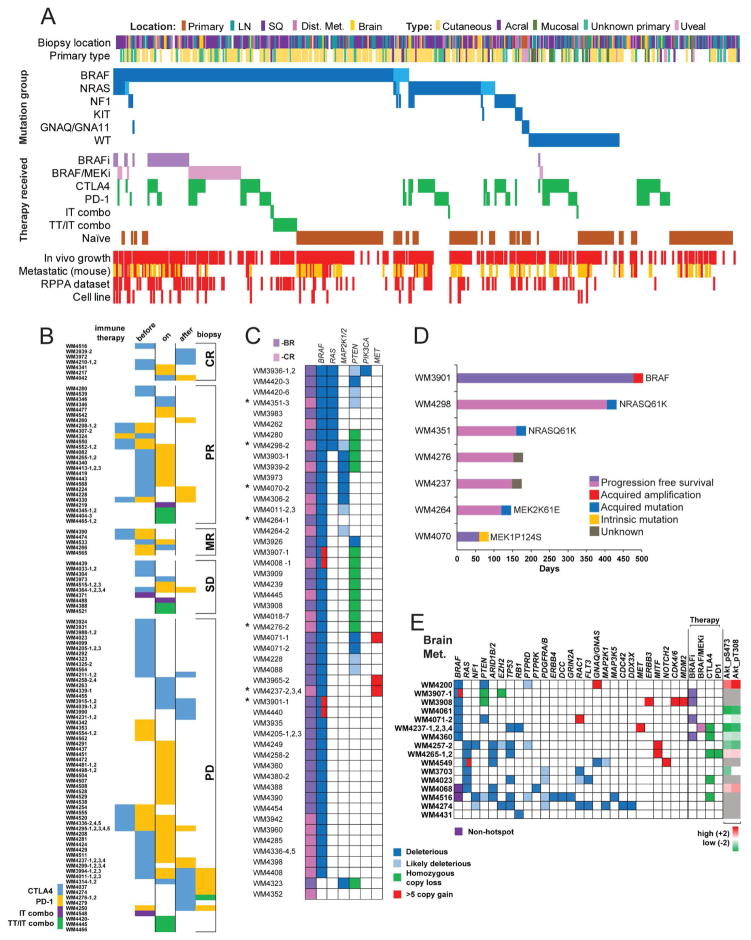
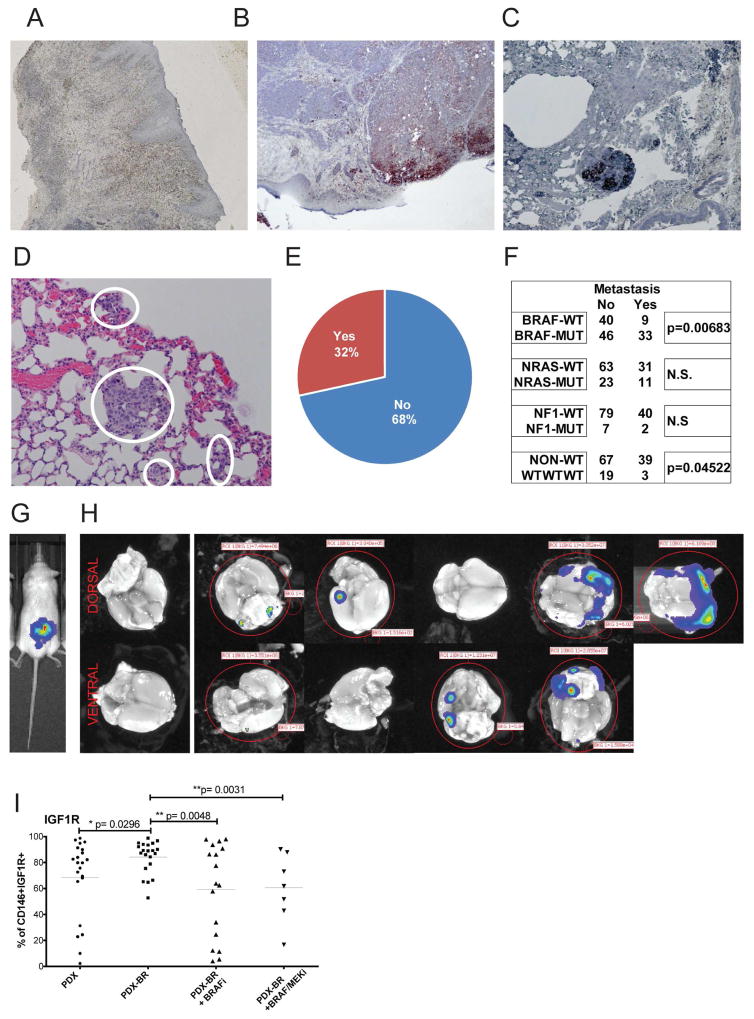
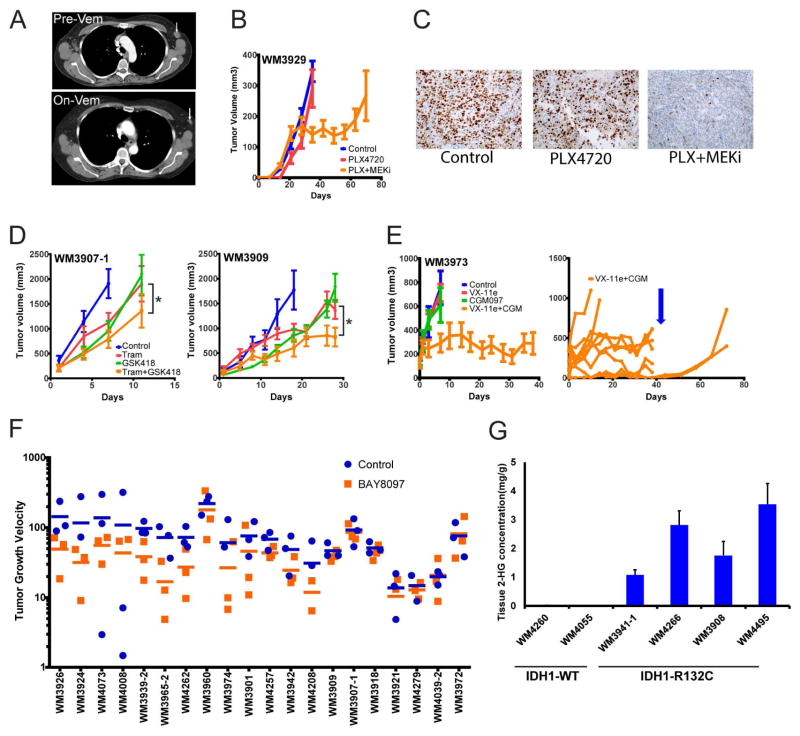
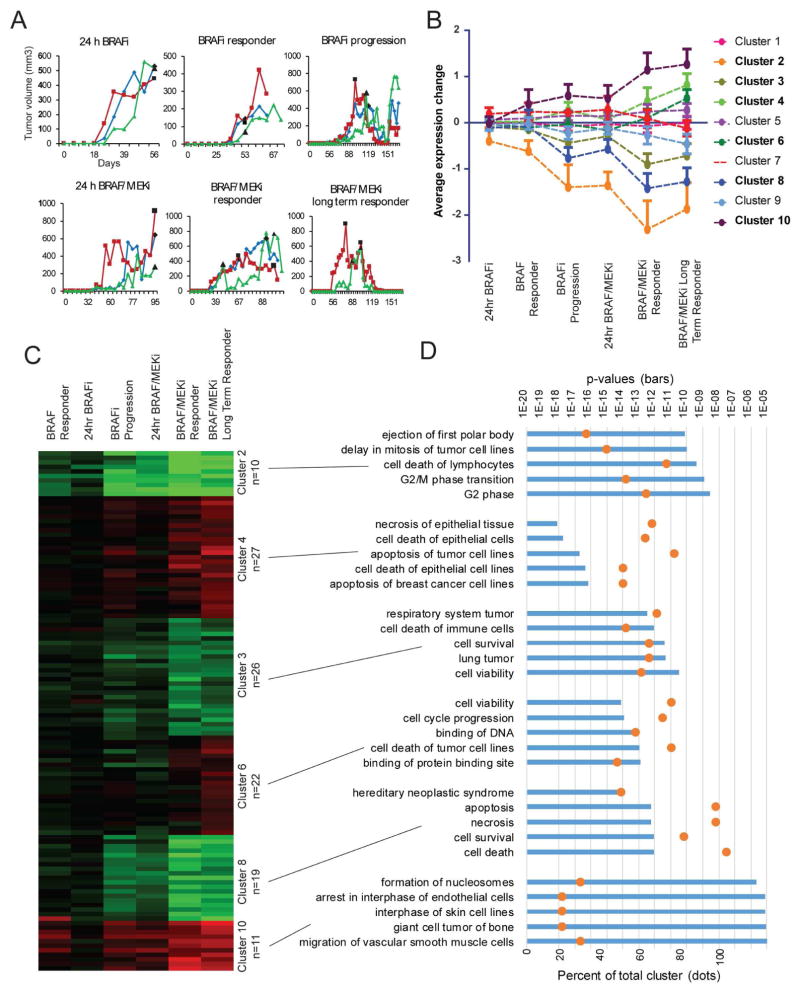
Therapy of advanced melanoma is changing dramatically. Following mutational and biological subclassification of this heterogeneous cancer, several targeted and immune therapies were approved and increased survival significantly. To facilitate further advancements through pre-clinical in vivo modeling, we have established 459 patient-derived xenografts (PDX) and live tissue samples from 384 patients representing the full spectrum of clinical, therapeutic, mutational, and biological heterogeneity of melanoma. PDX have been characterized using targeted sequencing and protein arrays and are clinically annotated. This exhaustive live tissue resource includes PDX from 57 samples resistant to targeted therapy, 61 samples from responders and non-responders to immune checkpoint blockade, and 31 samples from brain metastasis. Uveal, mucosal, and acral subtypes are represented as well. We show examples of pre-clinical trials that highlight how the PDX collection can be used to develop and optimize precision therapies, biomarkers of response, and the targeting of rare genetic subgroups.
Keywords: BRAF inhibitor resistance; ERK inhibitor; MDM2 inhibitor; PI3K beta inhibitor; immune checkpoint blockade; in vivo models; melanoma; melanoma brain metastasis; patient-derived xenografts; targeted therapy.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Bedard P, Tabernero J, Kurzrock R, Britten CD, Stathis A, Perez-Garcia JM, Zubel A, Le NT, Carter K, Bellew KM, et al. A phase lb, open-label, multicenter, dose-escalation study of the oral pan-PI3K inhibitor BKM120 in combination with the oral MEK1/2 inhibitor GSK1120212 in patients (pts) with selected advanced solid tumors. ASCO Meeting Abstracts. 2012;30:3003.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
