

DETECT I & DETECT II: a study protocol for a prospective multicentre observational study to validate the UroMark assay for the detection of bladder cancer from urinary cells
- PMID: 29141603
- PMCID: PMC5688623
- DOI: 10.1186/s12885-017-3758-7
DETECT I & DETECT II: a study protocol for a prospective multicentre observational study to validate the UroMark assay for the detection of bladder cancer from urinary cells
Abstract
Background: Haematuria is a common finding in general practice which requires visual inspection of the bladder by cystoscopy as well as upper tract imaging. In addition, patients with non-muscle invasive bladder cancer (NMIBC) often require surveillance cystoscopy as often as three monthly depending on disease risk. However, cystoscopy is an invasive procedure which is uncomfortable, requires hospital attendance and is associated with a risk of urinary tract infection. We have developed the UroMark assay, which can detect 150 methylation specific alteration specific to bladder cancer using DNA from urinary sediment cells.
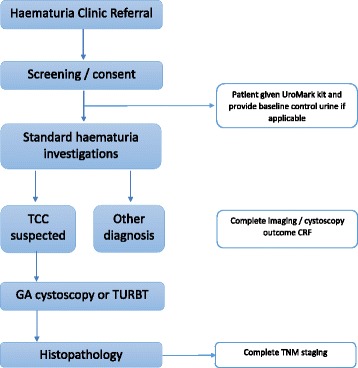
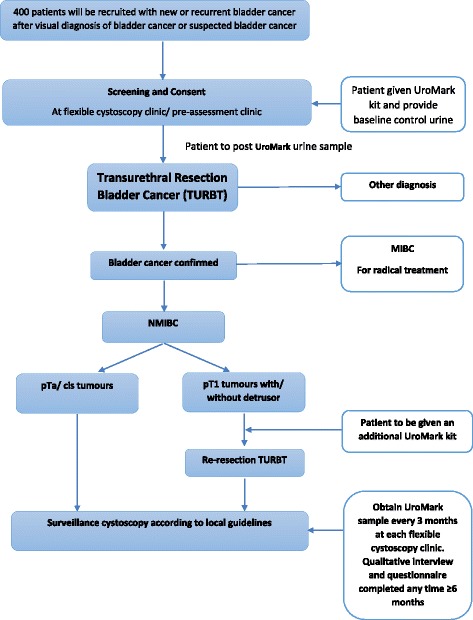
Methods: DETECT I and DETECT II are two multi-centre prospective observational studies designed to conduct a robust validation of the UroMark assay. DETECT I will recruit patients having diagnostic investigations for haematuria to determine the negative predictive value of the UroMark to rule out the presence of bladder cancer. DETECT II will recruit patients with new or recurrent bladder cancer to determine the sensitivity of the UroMark in detecting low, intermediate and high grade bladder cancer. NMIBC patients in DETECT II will be followed up with three monthly urine sample collection for 24 months while having surveillance cystoscopy. DETECT II will include a qualitative analysis of semi-structured interviews to explore patients' experience of being diagnosed with bladder cancer and having cystoscopy and a urinary test for bladder cancer surveillance. Results of the UroMark will be compared to cystoscopy findings and histopathological results in patients with bladder cancer.
Discussion: A sensitive and specific urinary biomarker will revolutionise the haematuria diagnostic pathway and surveillance strategies for NMIBC patients. None of the six approved US Food and Drug Administration urinary test are recommended as a standalone test. The UroMark assay is based on next generation sequencing technology which interrogates 150 loci and represents a step change compared to other biomarker panels. This enhances the sensitivity of the test and by using a random forest classifier approach, where the UroMark results are derived from a cut off generated from known outcomes of previous samples, addresses many shortcomings of previous assays.
Trial registration: Both trails are registered on clinicaltrials.gov.
Detect i: NCT02676180 (18th December 2015).
Detect ii: NCT02781428 (11th May 2016).
Keywords: Bladder cancer; Clinical trial; Diagnostic; Haematuria; Methylation; Next generation sequencing; Surveillance; Urinary assay; Urinary biomarker; Validation.
Conflict of interest statement
Ethics approval and consent to participate
DETECT I was approved by NHS Health Research Authority on the 18th May 2016 (IRAS project ID: 179,245, REC reference: 16/NW/0150,
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
