

Norethisterone enanthate-induced cerebral venous sinus thrombosis (CVST)
- PMID: 29141931
- PMCID: PMC5695460
- DOI: 10.1136/bcr-2017-222418
Norethisterone enanthate-induced cerebral venous sinus thrombosis (CVST)
Abstract
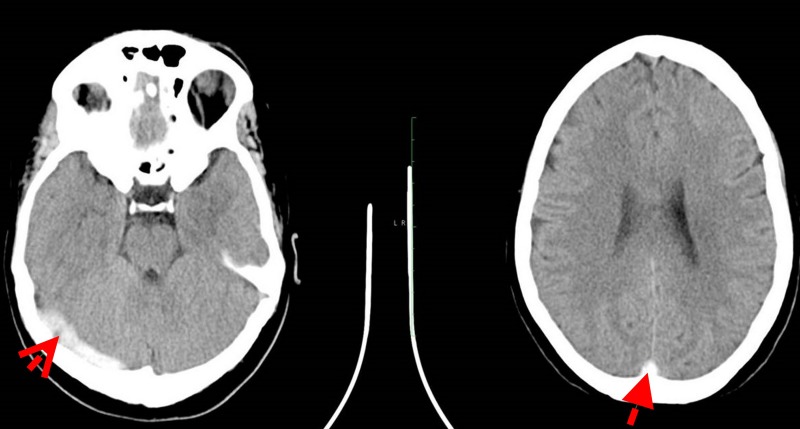
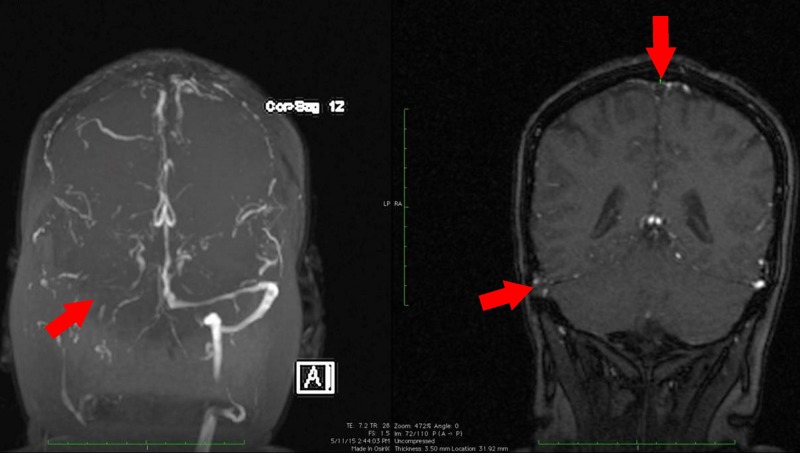
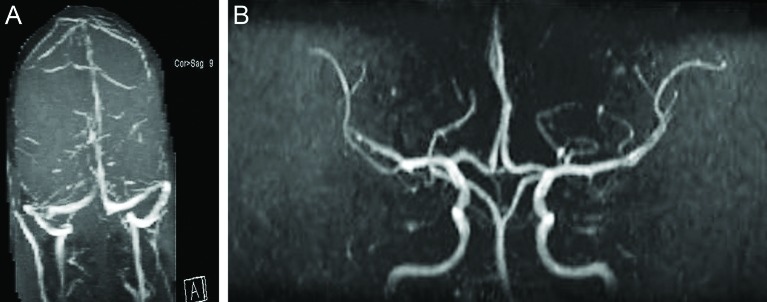
A 23-year-old East Indian woman with no significant medical history, except a depot-norethisterone enanthate injection taken 3 weeks prior to admission, presented with a gradually worsening headache for the past 5 days. She had no fever, vomiting, neck stiffness, focal weakness or rash, and examination was unremarkable with no focal neurological deficits. Vasculitic, thrombophilia and sepsis screens were normal. A brain CT scan showed a left parietal lobe venous infarct, secondary to a venous dural sinus thrombosis, with MRI and Magnetic Resonance Venogram (MRV) confirming a signal void. She was diagnosed to have multiple cerebral venous sinus thrombosis due to norethisterone enanthate. She made a complete recovery following treatment with mannitol, dexamethasone and anticoagulants. A follow-up brain MRI done at 6 months was normal.
Keywords: drugs and medicines; neurology (drugs and medicines).
© BMJ Publishing Group Ltd (unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Ramya T, Prakash B, Devi B. Norethisterone induced cerebral venous sinus thrombosis (CVST): a rare case report and review of literature. Int J Reprod Contracept Obstet Gynecol 2014;3:231–5.
-
- Rajput R, Dhuan J, Agarwal S. CVST in a young woman taking norethindrone acetate for DUB: a case report and review of literature. J Obstet Gynaecology Can 2008;30:680–3. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous