

Value of Progression of Coronary Artery Calcification for Risk Prediction of Coronary and Cardiovascular Events: Result of the HNR Study (Heinz Nixdorf Recall)
- PMID: 29142010
- PMCID: PMC5811240
- DOI: 10.1161/CIRCULATIONAHA.116.027034
Value of Progression of Coronary Artery Calcification for Risk Prediction of Coronary and Cardiovascular Events: Result of the HNR Study (Heinz Nixdorf Recall)
Abstract
Background: Computed tomography (CT) allows estimation of coronary artery calcium (CAC) progression. We evaluated several progression algorithms in our unselected, population-based cohort for risk prediction of coronary and cardiovascular events.
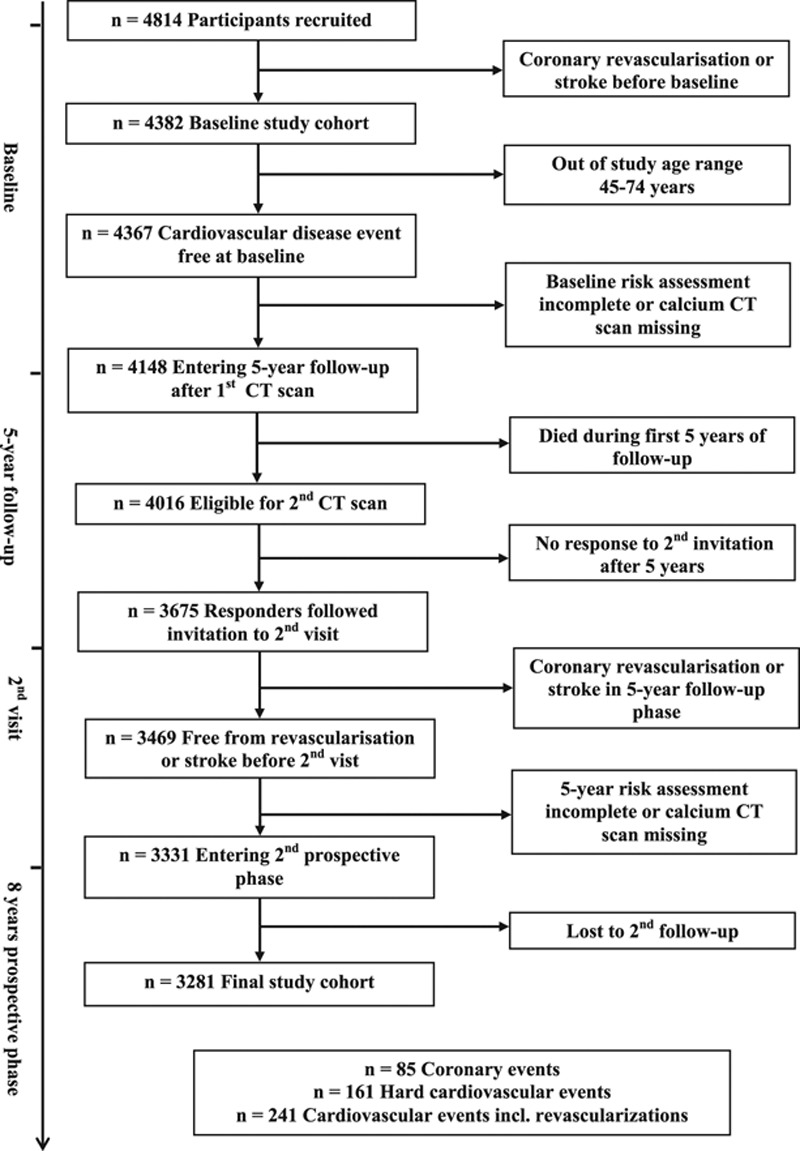
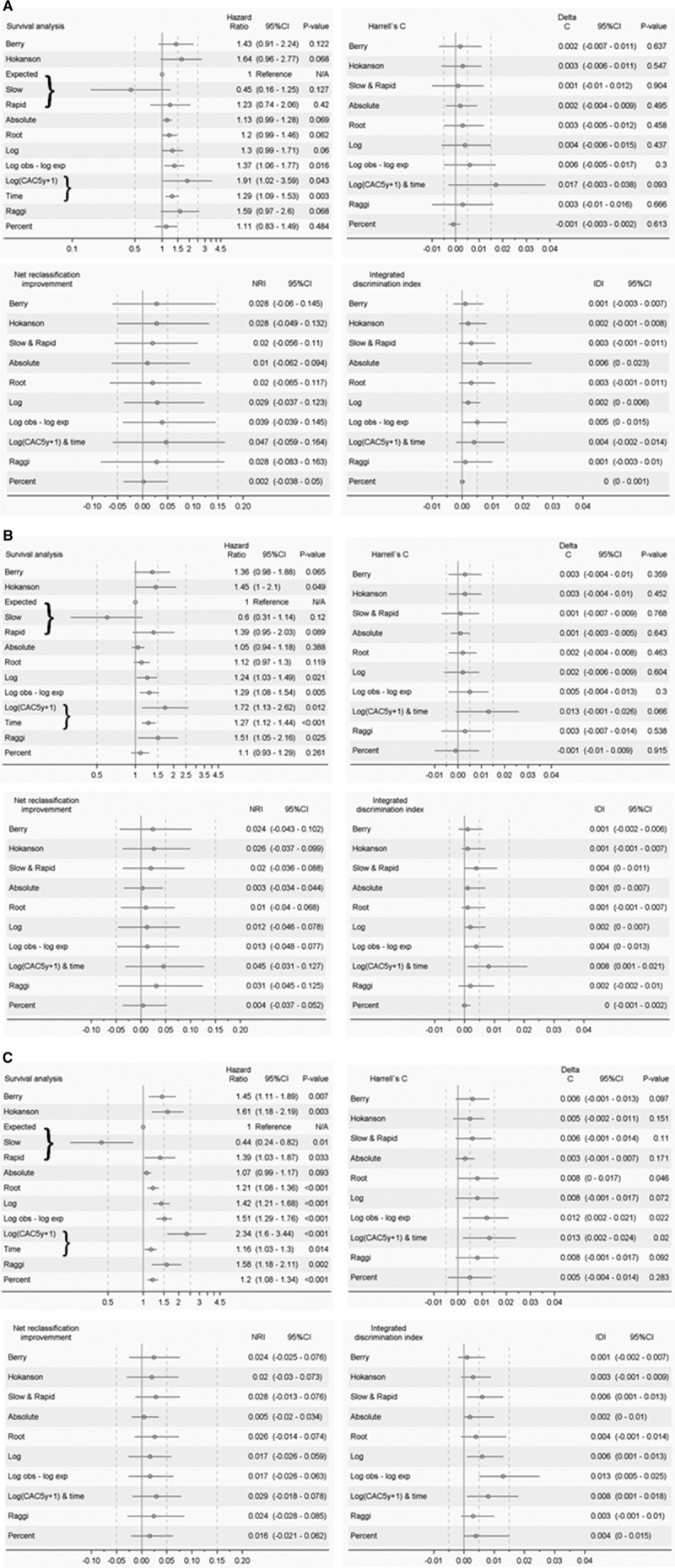
Methods: In 3281 participants (45-74 years of age), free from cardiovascular disease until the second visit, risk factors, and CTs at baseline (b) and after a mean of 5.1 years (5y) were measured. Hard coronary and cardiovascular events, and total cardiovascular events including revascularization, as well, were recorded during a follow-up time of 7.8±2.2 years after the second CT. The added predictive value of 10 CAC progression algorithms on top of risk factors including baseline CAC was evaluated by using survival analysis, C-statistics, net reclassification improvement, and integrated discrimination index. A subgroup analysis of risk in CAC categories was performed.
Results: We observed 85 (2.6%) hard coronary, 161 (4.9%) hard cardiovascular, and 241 (7.3%) total cardiovascular events. Absolute CAC progression was higher with versus without subsequent coronary events (median, 115 [Q1-Q3, 23-360] versus 8 [0-83], P<0.0001; similar for hard/total cardiovascular events). Some progression algorithms added to the predictive value of baseline CT and risk assessment in terms of C-statistic or integrated discrimination index, especially for total cardiovascular events. However, CAC progression did not improve models including CAC5y and 5-year risk factors. An excellent prognosis was found for 921 participants with double-zero CACb=CAC5y=0 (10-year coronary and hard/total cardiovascular risk: 1.4%, 2.0%, and 2.8%), which was for participants with incident CAC 1.8%, 3.8%, and 6.6%, respectively. When CACb progressed from 1 to 399 to CAC5y≥400, coronary and total cardiovascular risk were nearly 2-fold in comparison with subjects who remained below CAC5y=400. Participants with CACb≥400 had high rates of hard coronary and hard/total cardiovascular events (10-year risk: 12.0%, 13.5%, and 30.9%, respectively).
Conclusions: CAC progression is associated with coronary and cardiovascular event rates, but adds only weakly to risk prediction. What counts is the most recent CAC value and risk factor assessment. Therefore, a repeat scan >5 years after the first scan may be of additional value, except when a double-zero CT scan is present or when the subjects are already at high risk.
Keywords: atherosclerosis; coronary disease; disease progression; risk assessment; tomography; vascular calcification.
© 2017 The Authors.
Figures
Comment in
-
Coronary Artery Calcium: If Measuring Once Is Good, Is Twice Better?Circulation. 2018 Feb 13;137(7):680-683. doi: 10.1161/CIRCULATIONAHA.117.031951. Circulation. 2018. PMID: 29440196 No abstract available.
References
-
- Budoff MJ, Raggi P. Coronary artery disease progression assessed by electron-beam computed tomography. Am J Cardiol. 2001;88(2A):46E–50E. - PubMed
-
- Kronmal RA, McClelland RL, Detrano R, Shea S, Lima JA, Cushman M, Bild DE, Burke GL. Risk factors for the progression of coronary artery calcification in asymptomatic subjects: results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2007;115:2722–2730. doi: 10.1161/CIRCULATIONAHA.106.674143. - PubMed
-
- Erbel R, Lehmann N, Churzidse S, Rauwolf M, Mahabadi AA, Möhlenkamp S, Moebus S, Bauer M, Kälsch H, Budde T, Montag M, Schmermund A, Stang A, Führer-Sakel D, Weimar C, Roggenbuck U, Dragano N, Jöckel KH Heinz Nixdorf Recall Study Investigators. Progression of coronary artery calcification seems to be inevitable, but predictable: results of the Heinz Nixdorf Recall (HNR) study. Eur Heart J. 2014;35:2960–2971. doi: 10.1093/eurheartj/ehu288. - PMC - PubMed
-
- Schindler TH, Cadenas J, Facta AD, Li Y, Olschewski M, Sayre J, Goldin J, Schelbert HR. Improvement in coronary endothelial function is independently associated with a slowed progression of coronary artery calcification in type 2 diabetes mellitus. Eur Heart J. 2009;30:3064–3073. doi: 10.1093/eurheartj/ehp482. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
