

Using a quantitative quadruple immunofluorescent assay to diagnose isolated mitochondrial Complex I deficiency
- PMID: 29142257
- PMCID: PMC5688115
- DOI: 10.1038/s41598-017-14623-2
Using a quantitative quadruple immunofluorescent assay to diagnose isolated mitochondrial Complex I deficiency
Abstract
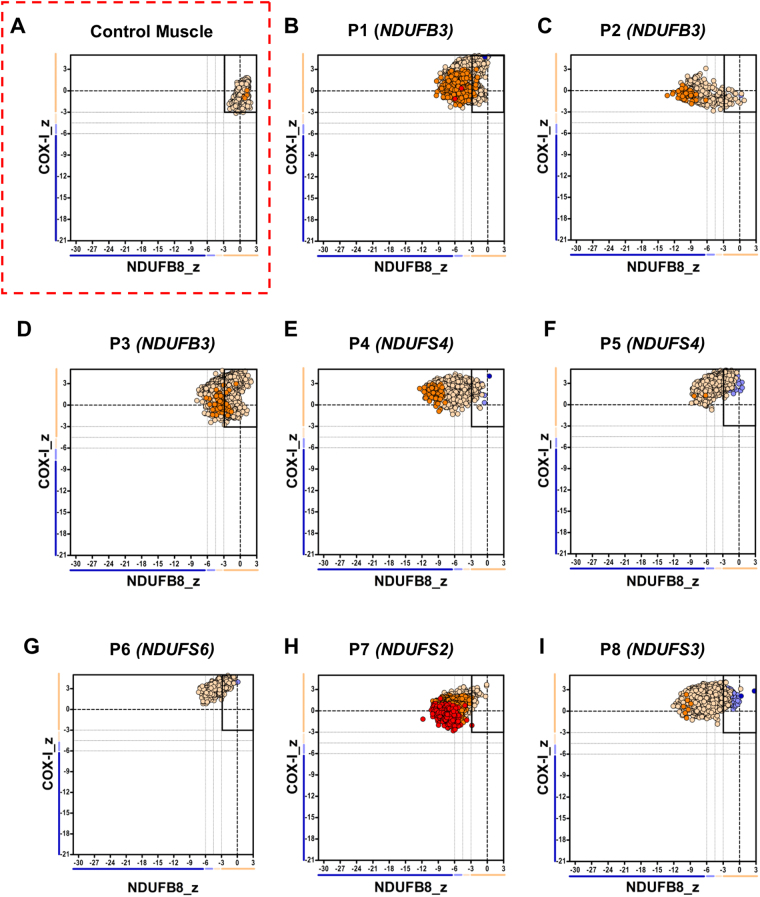
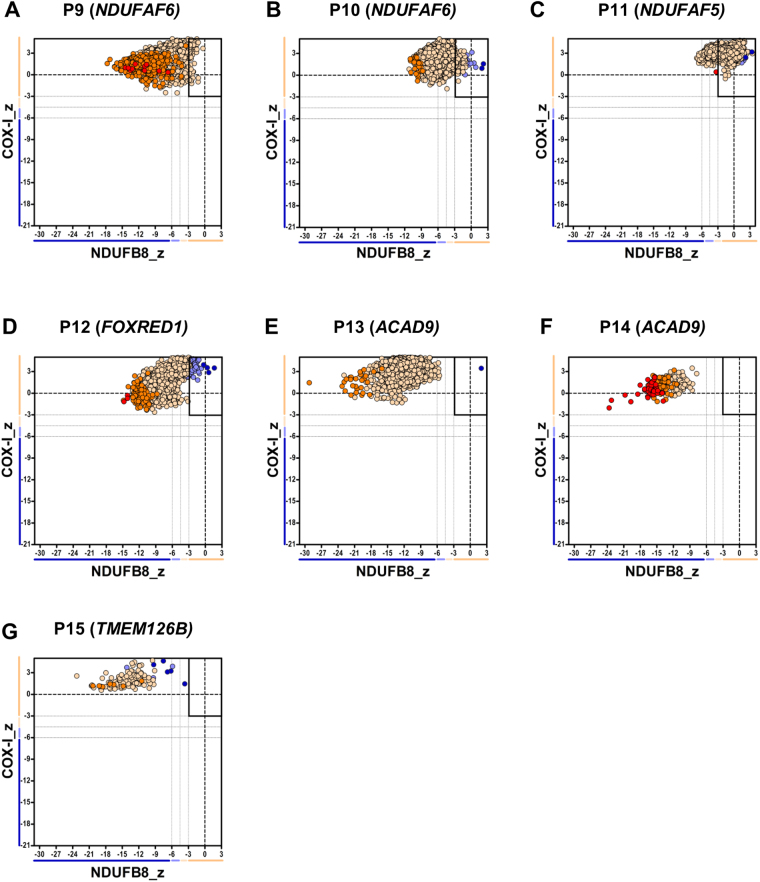
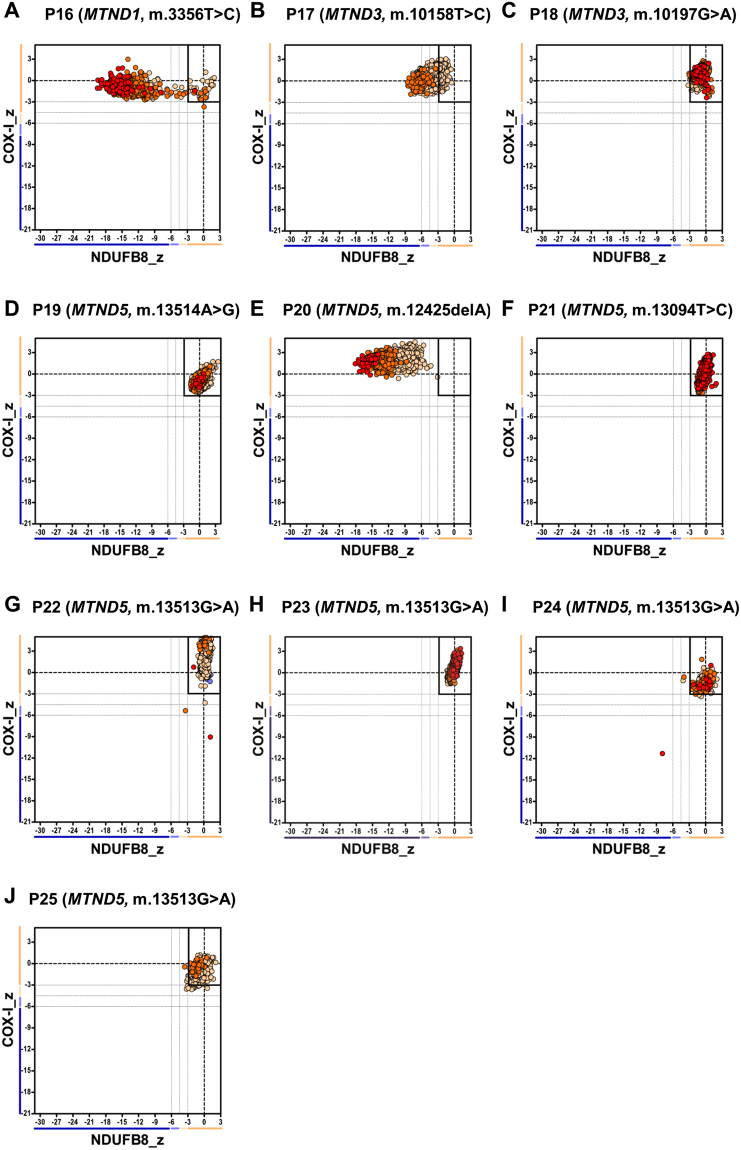
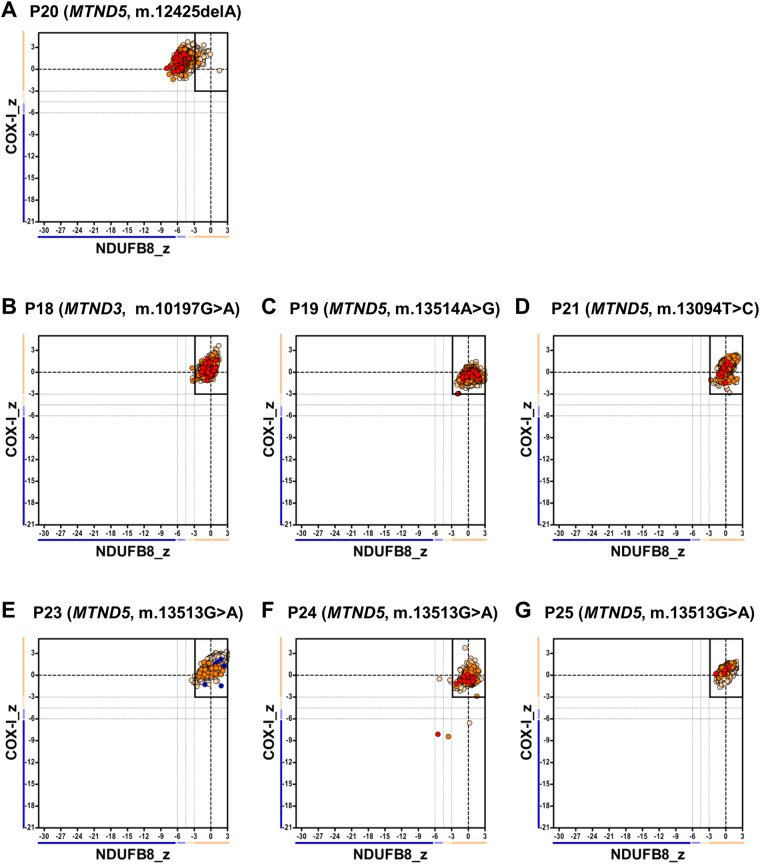
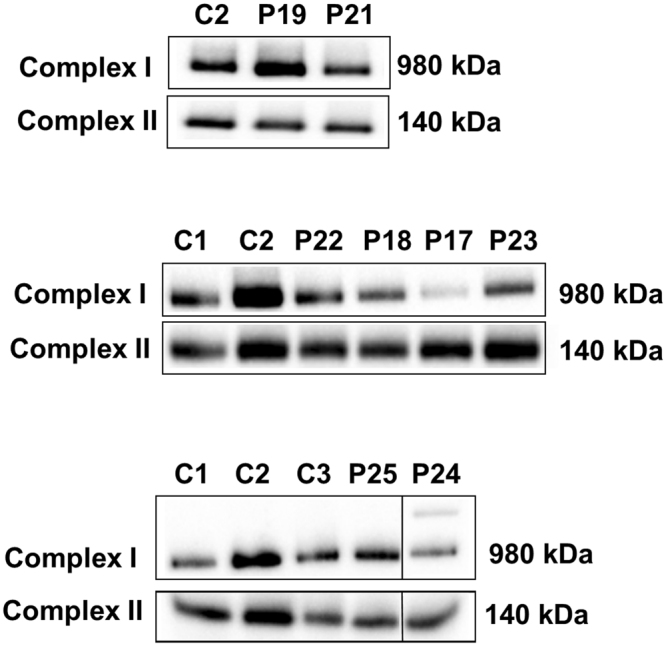
Isolated Complex I (CI) deficiency is the most commonly observed mitochondrial respiratory chain biochemical defect, affecting the largest OXPHOS component. CI is genetically heterogeneous; pathogenic variants affect one of 38 nuclear-encoded subunits, 7 mitochondrial DNA (mtDNA)-encoded subunits or 14 known CI assembly factors. The laboratory diagnosis relies on the spectrophotometric assay of enzyme activity in mitochondrially-enriched tissue homogenates, requiring at least 50 mg skeletal muscle, as there is no reliable histochemical method for assessing CI activity directly in tissue cryosections. We have assessed a validated quadruple immunofluorescent OXPHOS (IHC) assay to detect CI deficiency in the diagnostic setting, using 10 µm transverse muscle sections from 25 patients with genetically-proven pathogenic CI variants. We observed loss of NDUFB8 immunoreactivity in all patients with mutations affecting nuclear-encoding structural subunits and assembly factors, whilst only 3 of the 10 patients with mutations affecting mtDNA-encoded structural subunits showed loss of NDUFB8, confirmed by BN-PAGE analysis of CI assembly and IHC using an alternative, commercially-available CI (NDUFS3) antibody. The IHC assay has clear diagnostic potential to identify patients with a CI defect of Mendelian origins, whilst highlighting the necessity of complete mitochondrial genome sequencing in the diagnostic work-up of patients with suspected mitochondrial disease.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
