

" Who has to do it at the end of the day? Programme officials or hospital authorities?" Airborne infection control at drug resistant tuberculosis (DR-TB) centres of Karnataka, India: a mixed-methods study
- PMID: 29142744
- PMCID: PMC5674795
- DOI: 10.1186/s13756-017-0270-4
" Who has to do it at the end of the day? Programme officials or hospital authorities?" Airborne infection control at drug resistant tuberculosis (DR-TB) centres of Karnataka, India: a mixed-methods study
Abstract
Background: Drug resistant tuberculosis (DR-TB) centers admit patients with DR-TB for initiation of treatment and thereby concentrate the patients under one setting. It becomes imperative to assess the compliance of DR-TB centres to national airborne infection control (AIC) guidelines and explore the provider perspectives into reasons for unsatisfactory compliance.
Methods: This mixed methods study (triangulation design) was carried out across all the six DR-TB centers of Karnataka state, India, between November 2016 and April 2017. Non-participant observation using a structured format was carried out at the DR-TB wards (n = 6), outpatient departments (n = 6), patient waiting areas outside outpatient departments (n = 6) and culture and drug susceptibility testing laboratories (n = 3). Structured interviews of admitted patients (n = 30) were done to assess the knowledge on cough hygiene and sputum disposal. Key informant interviews (KIIs) of health care providers (n = 20) were done. Manual descriptive content analysis was done to analyse the transcripts of KIIs.
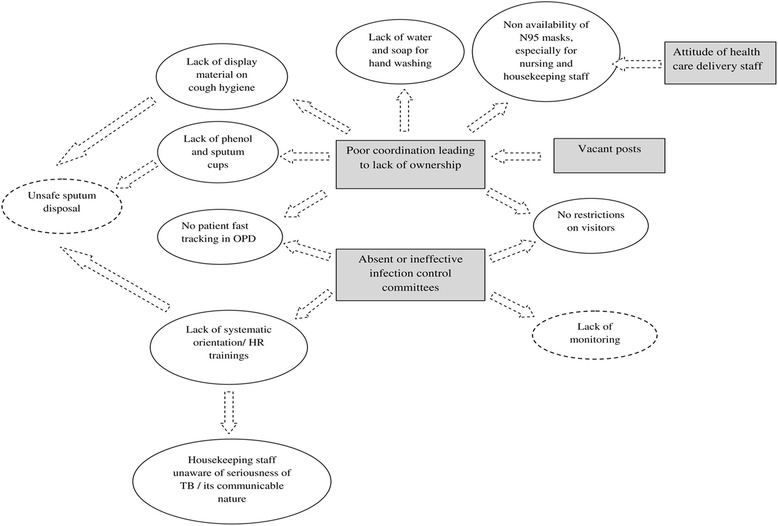
Results: The findings related to compliance in non-participant observation were corroborated by KIIs. All the laboratories were consistently implementing the AIC guidelines. Compliance to hand hygiene, wet mopping and ventilation measures were satisfactory in four or more DR-TB wards. The non-availability of N95 masks in wards as well as outpatient departments was staggering. Sputum disposal without prior disinfection and the lack of display materials on cough hygiene and patient education was common. Patient fast tracking in outpatient department waiting areas and visitor restrictions in wards were lacking. Trainings on AIC measures were uncommon. About half and one-third of patients admitted had satisfactory knowledge regarding sputum disposal and situations demanding mask respectively. The reasons for unsatisfactory compliance to AIC guidelines were poor coordination between programme and hospital authorities leading to lack of ownership; ineffective or non-existent infection control committees; vacant posts of medical officers; and attitudes of health care delivery staff.
Conclusion: Compliance with AIC guidelines in DR-TB centers of Karnataka was sub-optimal. The reasons identified require urgent attention of the programme managers and hospital authorities.
Keywords: Drug-resistant tuberculosis; Hospital infections; Infection control; MDR tuberculosis; SORT IT.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was obtained from the Institutional Ethics Committee of Yenepoya University, Mangaluru, India (protocol number YUEC/2016/288, approval dated 12/11/2016) and the Ethics Advisory Group of the International Union against Tuberculosis and Lung Disease (The Union), Paris, France (EAG No. 92/16 dated 17/10/2016). Written informed consent was taken from the relevant authorities for facility observation, the same was obtained from patients for structured interview and from health care providers for key informant interviews. Permission was taken from the Joint Director, Tuberculosis of the state of Karnataka before initiating the study. We decided against providing age of participant whose quotes were used to protect the identity of the participant. The investigator used N95 mask while interviewing the patients and assessing the AIC compliance in DR-TB centers.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- World Health Organization. Global TB Report 2016. Geneva; 2016. Available at http://apps.who.int/iris/bitstream/10665/250441/1/9789241565394-eng.pdf?.... Accessed 14 June 2017.
-
- Central TB Division Directorate General of Health Services Ministry of Health and Family Welfare. TB India 2017. New Delhi; 2017. Available at https://tbcindia.gov.in/WriteReadData/TB%20India%202017.pdf. Accessed 14 June 2017.
-
- Central TB Division Directorate General of Health Services Ministry of Health and Family Welfare. Guidelines on Programmatic Management of Drug Resistant TB (PMDT) in India. New Delhi; 2012. Available at https://tbcindia.gov.in/WriteReadData/l892s/8320929355Guidelines%20for%2.... Accessed 13 Sept 2016.
-
- Jarand J, Shean K, O’Donnell M, Loveday M, Kvasnovsky C, Van der Walt M, et al. Extensively drug-resistant tuberculosis (XDR-TB) among health care workers in South Africa. Trop. Med. Int Heal. 2010;15:1179–1184. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
