

The application of drains in thyroid surgery
- PMID: 29142849
- PMCID: PMC5676181
- DOI: 10.21037/gs.2017.07.04
The application of drains in thyroid surgery
Abstract
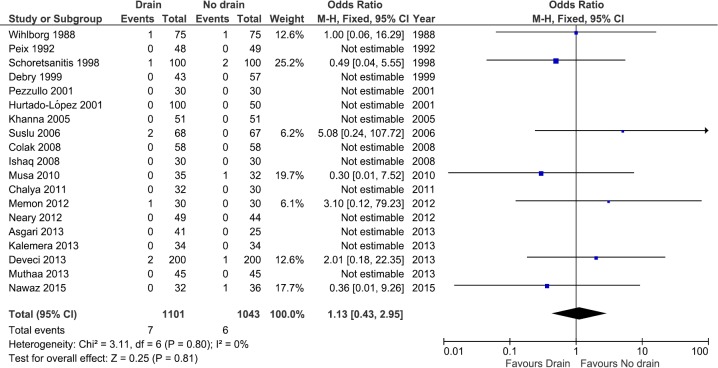
It has been shown that the use of drain in thyroid surgery does not reduce the reoperation rate for hemorrhage. The aim of this systematic review was to update the knowledge of the role of drain in thyroid surgery in term of postoperative complications, pain and hospital length of stay (LOS). A systematic search was performed in the PubMed and Embase database to identify all randomized controlled trials (RCTs) comparing clinical outcomes in patients who underwent thyroidectomy or lobectomy with or without drainage. The primary outcome was reoperation rate for bleeding; the secondary outcomes were development of hematoma, seroma, and wound infection; postoperative pain evaluated by Visual Analogue Scale (VAS) at the postoperative day (POD) 1, and hospital LOS. Risk ratios (RRs) and 95% confident intervals (95% CI) were used for dichotomous variables; mean differences (MDs) and 95% CI for continuous variables. Statistical heterogeneity was evaluated and its degree was quantified by the I2 statistic. Twenty RCTs were included, with 2,204 patients enrolled. No difference was found between the two groups in term of reoperation [RR 1.13 (0.43, 2.95); I2 =0%], hematoma [RR 1.18 (0.71, 1.95); I2 =0%], and seroma [RR 0.82 (0.44, 1.53); I2 =0%]. Patients with drain had higher postoperative pain [MD 1.91 (1.30, 2.53); I2 =97%], prolonged hospital LOS [MD 1.34 (0.91, 1.76) days; I2 =98%], and increased wound infection rate [RR 2.82 (1.36, 5.86); I2 =0%], even though the latter was not confirmed in the sensitivity analysis including only studies with ≥100 patients per trial. The use of drain after thyroid surgery increase postoperative pain and hospital LOS, with no decrease of reoperation rate, hematoma and seroma formation. An increased wound infection rate in patients with drain is suggested, but a large RCT should be performed to confirm this correlation.
Keywords: Drainage; meta-analysis; postoperative complications; randomized controlled trial (RCT); thyroidectomy.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures









Similar articles
-
Comparison of drain versus no-drain thyroidectomy: a meta-analysis.Eur Arch Otorhinolaryngol. 2017 Jan;274(1):567-577. doi: 10.1007/s00405-016-4213-0. Epub 2016 Jul 28. Eur Arch Otorhinolaryngol. 2017. PMID: 27470116
-
Systematic review and meta-analysis of the use of high-energy devices for thyroid surgery.Langenbecks Arch Surg. 2024 Jul 17;409(1):217. doi: 10.1007/s00423-024-03399-5. Langenbecks Arch Surg. 2024. PMID: 39017727
-
Drainage after total thyroidectomy or lobectomy for benign thyroidal disorders.J Zhejiang Univ Sci B. 2008 Apr;9(4):319-23. doi: 10.1631/jzus.B0720257. J Zhejiang Univ Sci B. 2008. PMID: 18381807 Free PMC article. Clinical Trial.
-
To drain or not to drain after thyroid surgery: a randomized controlled trial at a tertiary Hospital in East Africa.Afr Health Sci. 2013 Sep;13(3):748-55. doi: 10.4314/ahs.v13i3.33. Afr Health Sci. 2013. PMID: 24250317 Free PMC article. Clinical Trial.
-
Single versus double chest drains after pulmonary lobectomy: a systematic review and meta-analysis.World J Surg Oncol. 2020 Jul 20;18(1):175. doi: 10.1186/s12957-020-01945-1. World J Surg Oncol. 2020. PMID: 32690055 Free PMC article.
Cited by
-
Predictors and Preventive Strategies of Bleeding After Thyroid Surgery.Cureus. 2023 Oct 24;15(10):e47575. doi: 10.7759/cureus.47575. eCollection 2023 Oct. Cureus. 2023. PMID: 38021981 Free PMC article. Review.
-
Impact of drains on nausea and vomiting after thyroid and parathyroid surgery: a randomized controlled trial.Langenbecks Arch Surg. 2019 Sep;404(6):693-701. doi: 10.1007/s00423-019-01799-6. Epub 2019 Jun 26. Langenbecks Arch Surg. 2019. PMID: 31243574 Clinical Trial.
-
To drain or not to drain following thyroidectomy.: A prospective, randomized study.Saudi Med J. 2023 May;44(5):518-521. doi: 10.15537/smj.2023.44.5.20220031. Saudi Med J. 2023. PMID: 37182919 Free PMC article. Clinical Trial.
-
The effect of fibrin glue on the quantity of drainage after thyroidectomy: a randomized controlled pilot trial.Ann Surg Treat Res. 2022 Apr;102(4):177-184. doi: 10.4174/astr.2022.102.4.177. Epub 2022 Apr 5. Ann Surg Treat Res. 2022. PMID: 35475227 Free PMC article.
-
A clinical comparative study of thyroid surgeries with and without drain.Indian J Otolaryngol Head Neck Surg. 2023 Sep;75(3):1681-1686. doi: 10.1007/s12070-023-03700-w. Epub 2023 Mar 25. Indian J Otolaryngol Head Neck Surg. 2023. PMID: 37636765 Free PMC article.
References
-
- Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0. The Cochrane Collaboration 2011.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous