

The Unappreciated Role of Extrarenal and Gut Sensors in Modulating Renal Potassium Handling: Implications for Diagnosis of Dyskalemias and Interpreting Clinical Trials
- PMID: 29142913
- PMCID: PMC5678840
- DOI: 10.1016/j.ekir.2016.03.001
The Unappreciated Role of Extrarenal and Gut Sensors in Modulating Renal Potassium Handling: Implications for Diagnosis of Dyskalemias and Interpreting Clinical Trials
Abstract
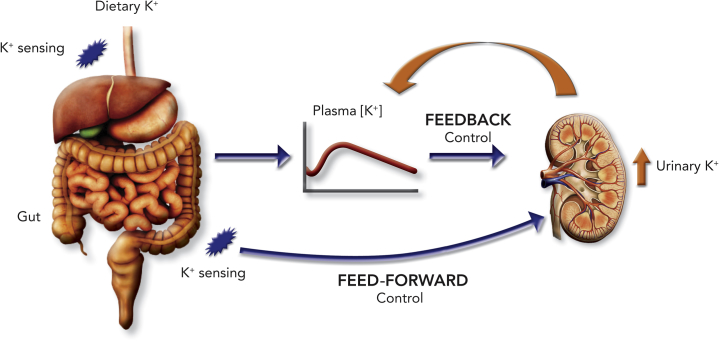
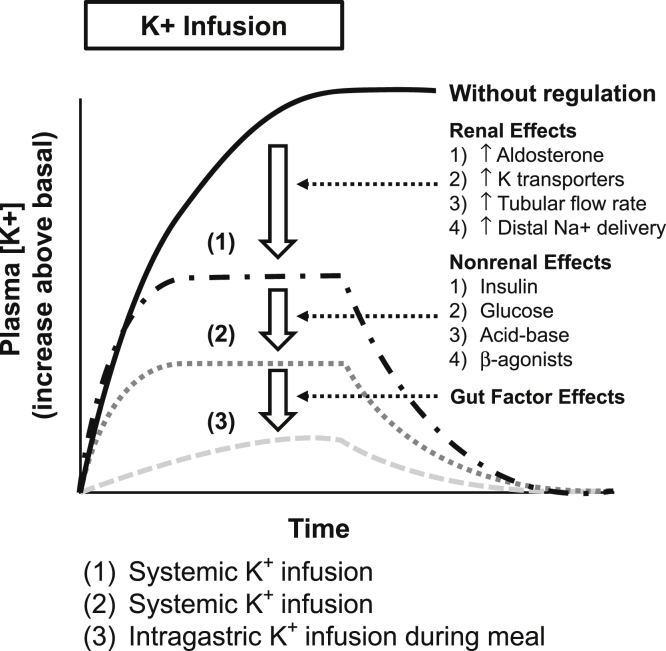
In addition to the classic and well-established "feedback control" of potassium balance, increasing investigative attention has focused on a novel and not widely recognized complementary regulatory paradigm for maintaining potassium homeostasis-the "feed-forward control" of potassium balance. This regulatory mechanism, initially defined in rumen, has recently been validated in normal human subjects. Studies are being conducted to determine the location for this putative potassium sensor and to evaluate potential signals, which might increase renal potassium excretion. Awareness of this more updated integrative control mechanism for potassium homeostasis is ever more relevant today, when the medical community is increasingly focused on the challenges of managing the hyperkalemia provoked by renin-angiotensin-aldosterone system inhibitors (RAASis). Recent studies have demonstrated a wide gap between RAASi prescribing guidelines and real-world experience and have highlighted that this gap is thought to be attributable in great part to hyperkalemia. Consequently we require a greater knowledge of the complexities of the regulatory mechanisms subserving potassium homeostasis. Sodium polystyrene sulfonate has long been the mainstay for treating hyperkalemia, but its administration is fraught with challenges related to patient discomfort and colonic necrosis. The current and imminent availability of newer potassium binders with better tolerability and more predictive dose-response potassium removal should enhance the management of hyperkalemia. Consequently it is essential to better understand the intricacies of mammalian colonic K+ handling. We discuss colonic transport of K+ and review evidence for potassium (BK) channels being responsible for increased stool K+ in patients with diseases such as ulcerative colitis.
Keywords: chronic kidney disease; potassium.
Figures
References
-
- Epstein M., Reaven N.L., Funk S.E. Evaluation of the treatment gap between clinical guidelines and the utilization of renin-angiotensin-aldosterone system inhibitors. Am J Manag Care. 2015;21(suppl):S212–S220. - PubMed
-
- Kosiborod M., Rasmussen H.S., Lavin P. Effect of sodium zirconium cyclosilicate on potassium lowering for 28 days among outpatients with hyperkalemia: the HARMONIZE randomized clinical trial. JAMA. 2014;312:2223–2233. - PubMed
-
- Packham D.K., Rasmussen H.S., Lavin P. Sodium zirconium cyclosilicate in hyperkalemia. N Engl J Med. 2015;372:222–231. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
