

Translating aetiological insight into sustainable management of type 2 diabetes
- PMID: 29143063
- PMCID: PMC6448962
- DOI: 10.1007/s00125-017-4504-z
Translating aetiological insight into sustainable management of type 2 diabetes
Abstract
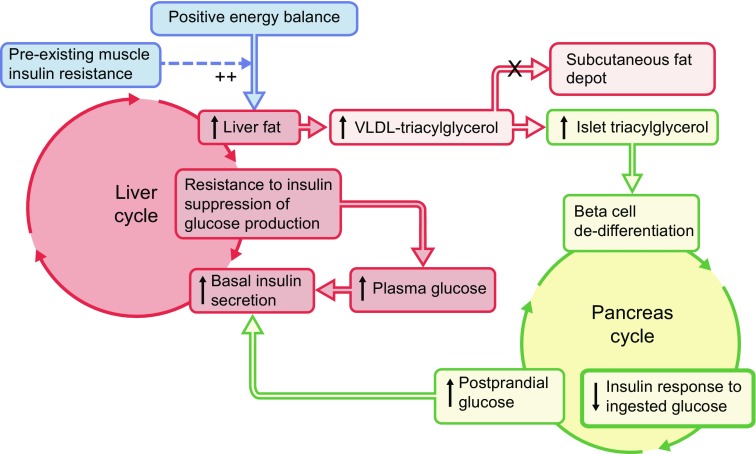
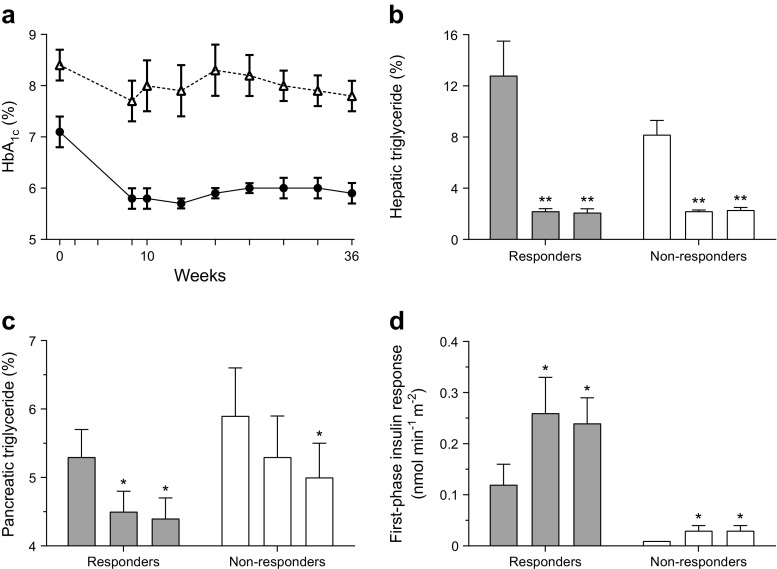
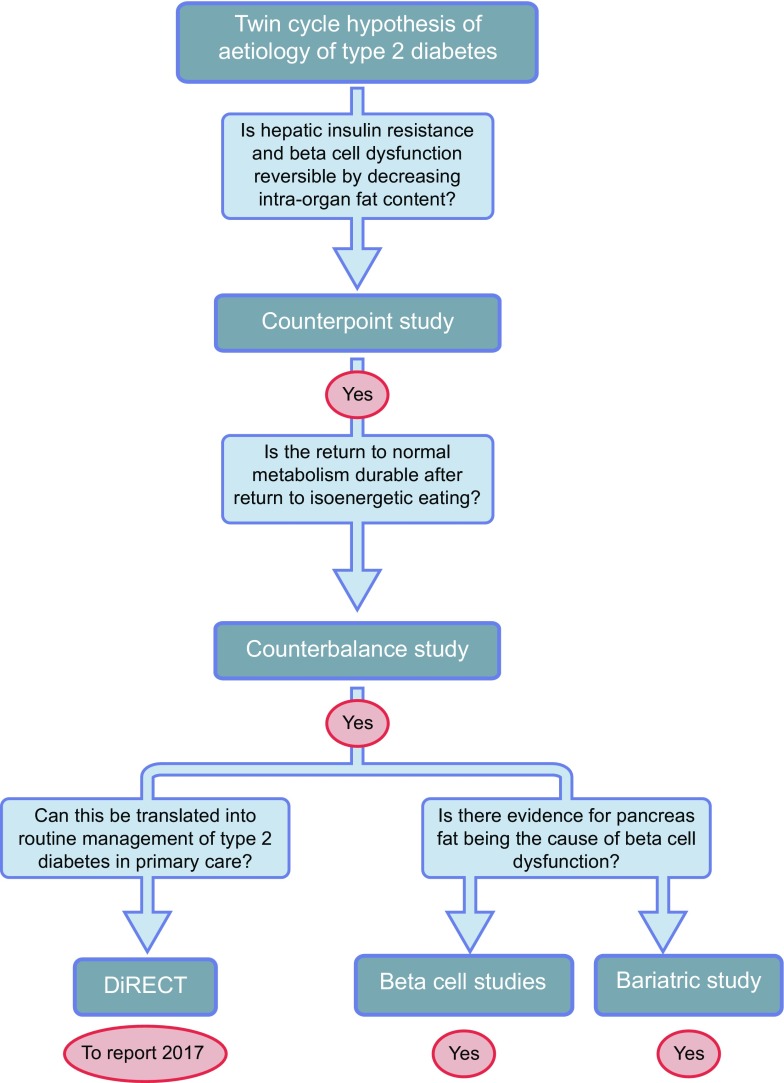
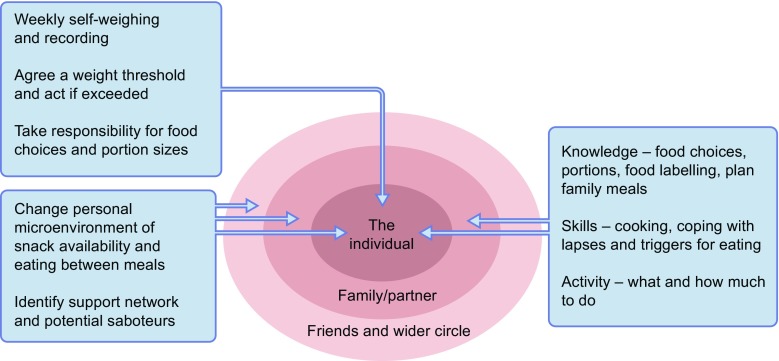
Using a low-energy diet as a tool, it has been possible to elucidate the sequence of pathophysiological changes that lead to the onset of type 2 diabetes. Negative energy balance in type 2 diabetes causes a profound fall in liver fat content resulting in normalisation of hepatic insulin sensitivity within 7 days. As the period of negative energy balance extends and liver fat levels fall to low normal, the rate of export of triacylglycerol from the liver falls. Consequent to this, the raised pancreas fat content falls and in early type 2 diabetes, normal first-phase insulin secretion becomes re-established with normal plasma glucose control. This research, driven by the predictions of the 2008 twin cycle hypothesis, has led to a paradigm shift in understanding. Studying the reversed sequence of pathophysiological changes, the linked abnormalities in liver and pancreas have been revealed. Early type 2 diabetes is a potentially reversible condition. Surprisingly, it was observed that the diet devised as an experimental tool was actually liked by research participants. It was associated neither with hunger nor tiredness in most people, but with rapidly increased wellbeing. A defined period of weight loss followed by carefully planned weight maintenance-the 'One, Two' approach-has since been applied in clinical practice. Motivated individuals can reverse their type 2 diabetes and remain normoglycaemic over years. A large study is underway to evaluate the applicability of this general approach to routine primary care practice as a long-term management strategy.
Keywords: Aetiology; Beta cell function; Liver fat; Low-energy diet; Management; Pancreas fat; Pathophysiology; Type 2 diabetes; Weight loss; Weight maintenance.
Conflict of interest statement
Duality of interest
The authors declare that there is no duality of interest associated with this manuscript.
Contribution statement
Both authors were responsible for drafting the article and revising it critically for important intellectual content. Both authors approved the version to be published.
Figures
References
-
- Schwarz JM, Linfoot P, Dare D, Aghajanian K. Hepatic de novo lipogenesis in normoinsulinemic and hyperinsulinemic subjects consuming high-fat, low-carbohydrate and low-fat, high-carbohydrate isoenergetic diets. Am J Clin Nutr. 2003;77:43–50. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
