

Modelling stillbirth mortality reduction with the Lives Saved Tool
- PMID: 29143647
- PMCID: PMC5688483
- DOI: 10.1186/s12889-017-4742-5
Modelling stillbirth mortality reduction with the Lives Saved Tool
Abstract
Background: The worldwide burden of stillbirths is large, with an estimated 2.6 million babies stillborn in 2015 including 1.3 million dying during labour. The Every Newborn Action Plan set a stillbirth target of ≤12 per 1000 in all countries by 2030. Planning tools will be essential as countries set policy and plan investment to scale up interventions to meet this target. This paper summarises the approach taken for modelling the impact of scaling-up health interventions on stillbirths in the Lives Saved tool (LiST), and potential future refinements.
Methods: The specific application to stillbirths of the general method for modelling the impact of interventions in LiST is described. The evidence for the effectiveness of potential interventions to reduce stillbirths are reviewed and the assumptions of the affected fraction of stillbirths who could potentially benefit from these interventions are presented. The current assumptions and their effects on stillbirth reduction are described and potential future improvements discussed.
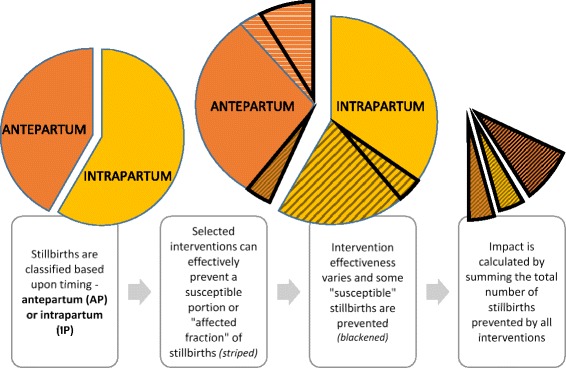
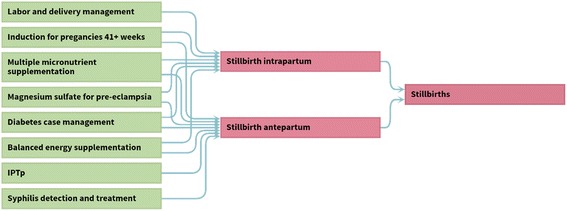
Results: High quality evidence are not available for all parameters in the LiST stillbirth model. Cause-specific mortality data is not available for stillbirths, therefore stillbirths are modelled in LiST using an attributable fraction approach by timing of stillbirths (antepartum/ intrapartum). Of 35 potential interventions to reduce stillbirths identified, eight interventions are currently modelled in LiST. These include childbirth care, induction for prolonged pregnancy, multiple micronutrient and balanced energy supplementation, malaria prevention and detection and management of hypertensive disorders of pregnancy, diabetes and syphilis. For three of the interventions, childbirth care, detection and management of hypertensive disorders of pregnancy, and diabetes the estimate of effectiveness is based on expert opinion through a Delphi process. Only for malaria is coverage information available, with coverage estimated using expert opinion for all other interventions. Going forward, potential improvements identified include improving of effectiveness and coverage estimates for included interventions and addition of further interventions.
Conclusions: Known effective interventions have the potential to reduce stillbirths and can be modelled using the LiST tool. Data for stillbirths are improving. Going forward the LiST tool should seek, where possible, to incorporate these improving data, and to continually be refined to provide an increasingly reliable tool for policy and programming purposes.
Keywords: Lives saved tool; Mortality modelling; Stillbirths.
Conflict of interest statement
Ethics approval and consent to participate
N/A.
Consent for publication
N/A.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Expanding the population coverage of evidence-based interventions with community health workers to save the lives of mothers and children: an analysis of potential global impact using the Lives Saved Tool (LiST).J Glob Health. 2017 Dec;7(2):020401. doi: 10.7189/jogh.07.020401. J Glob Health. 2017. PMID: 28959436 Free PMC article.
-
An analysis of three levels of scaled-up coverage for 28 interventions to avert stillbirths and maternal, newborn and child mortality in 27 countries in Latin America and the Caribbean with the Lives Saved Tool (LiST).BMC Public Health. 2016 Jul 22;16:613. doi: 10.1186/s12889-016-3238-z. BMC Public Health. 2016. PMID: 27443628 Free PMC article.
-
Triple return on investment: the cost and impact of 13 interventions that could prevent stillbirths and save the lives of mothers and babies in South Africa.BMC Pregnancy Childbirth. 2015 Feb 18;15:39. doi: 10.1186/s12884-015-0456-9. BMC Pregnancy Childbirth. 2015. PMID: 25879579 Free PMC article.
-
Delivering interventions to reduce the global burden of stillbirths: improving service supply and community demand.BMC Pregnancy Childbirth. 2009 May 7;9 Suppl 1(Suppl 1):S7. doi: 10.1186/1471-2393-9-S1-S7. BMC Pregnancy Childbirth. 2009. PMID: 19426470 Free PMC article. Review.
-
State of neonatal health care in eight countries of the SAARC region, South Asia: how can we make a difference?Paediatr Int Child Health. 2015 Aug;35(3):174-86. doi: 10.1179/2046905515Y.0000000046. Epub 2015 Jul 27. Paediatr Int Child Health. 2015. PMID: 26212573 Review.
Cited by
-
Identification of factors associated with stillbirth in Zimbabwe - a cross sectional study.BMC Pregnancy Childbirth. 2021 Sep 29;21(1):662. doi: 10.1186/s12884-021-04102-y. BMC Pregnancy Childbirth. 2021. PMID: 34587922 Free PMC article.
-
Prioritization of interventions in pursuit of maternal health policy objectives to mitigate stillbirth risks. An exploratory qualitative study at subnational level in Uganda.BMC Health Serv Res. 2021 Jan 11;21(1):53. doi: 10.1186/s12913-020-06046-z. BMC Health Serv Res. 2021. PMID: 33430858 Free PMC article.
-
Potential impact of midwives in preventing and reducing maternal and neonatal mortality and stillbirths: a Lives Saved Tool modelling study.Lancet Glob Health. 2021 Jan;9(1):e24-e32. doi: 10.1016/S2214-109X(20)30397-1. Epub 2020 Dec 1. Lancet Glob Health. 2021. PMID: 33275948 Free PMC article.
-
Projecting the impact of a national strategy to accelerate stunting prevention in East Nusa Tenggara, Indonesia, using the Lives Saved Tool.Narra J. 2025 Apr;5(1):e1462. doi: 10.52225/narra.v5i1.1462. Epub 2025 Jan 10. Narra J. 2025. PMID: 40352193 Free PMC article.
-
Stillbirth risk prediction using machine learning for a large cohort of births from Western Australia, 1980-2015.Sci Rep. 2020 Mar 24;10(1):5354. doi: 10.1038/s41598-020-62210-9. Sci Rep. 2020. PMID: 32210300 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
