

Effects of Aging on Fracture Healing
- PMID: 29143915
- PMCID: PMC6517062
- DOI: 10.1007/s11914-017-0413-9
Effects of Aging on Fracture Healing
Abstract
Purpose of review: This review summarizes research on the physiological changes that occur with aging and the resulting effects on fracture healing.
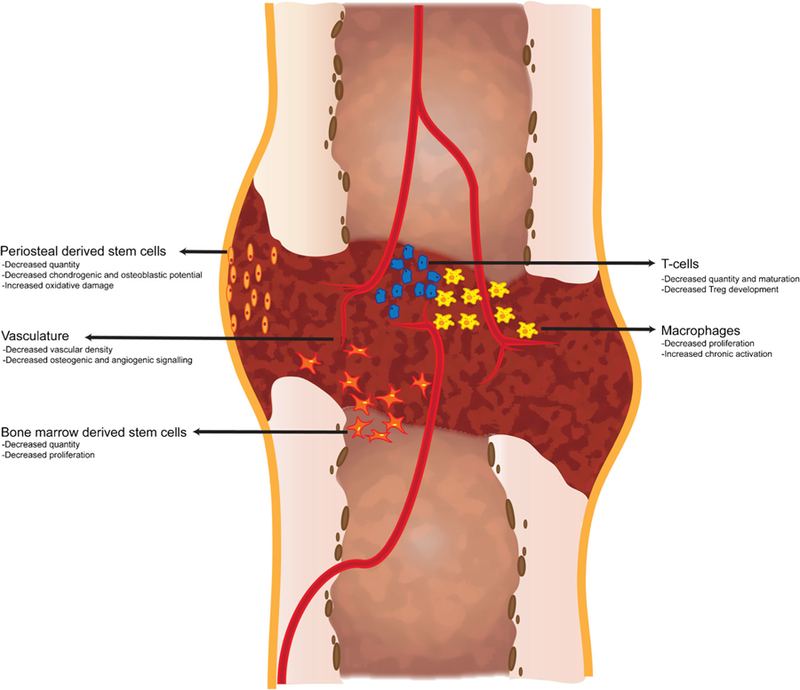
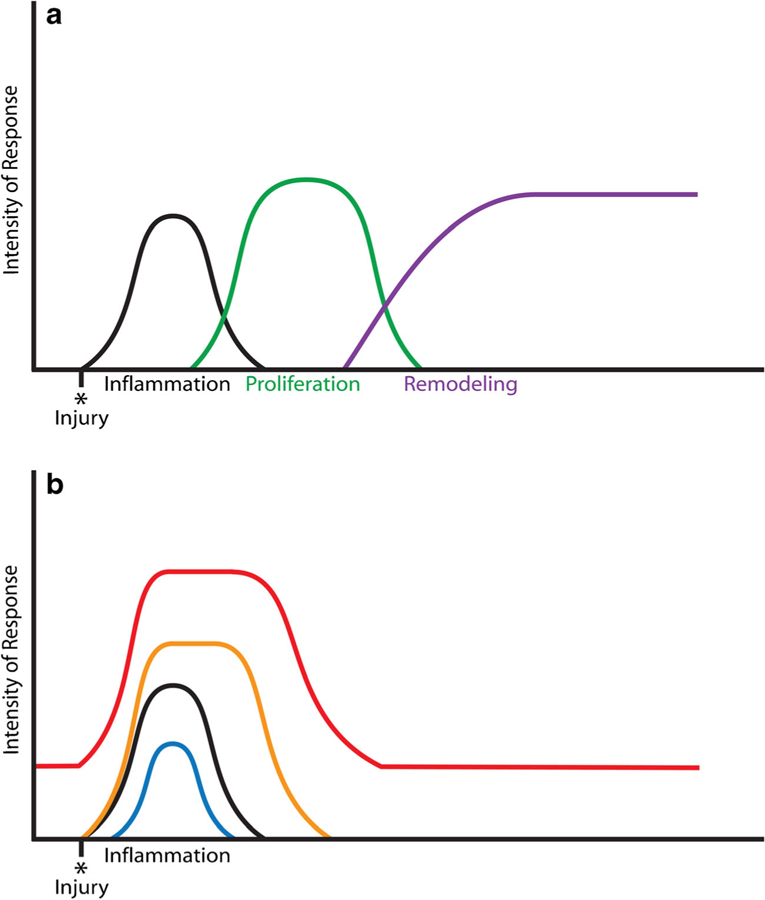
Recent findings: Aging affects the inflammatory response during fracture healing through senescence of the immune response and increased systemic pro-inflammatory status. Important cells of the inflammatory response, macrophages, T cells, mesenchymal stem cells, have demonstrated intrinsic age-related changes that could impact fracture healing. Additionally, vascularization and angiogenesis are impaired in fracture healing of the elderly. Finally, osteochondral cells and their progenitors demonstrate decreased activity and quantity within the callus. Age-related changes affect many of the biologic processes involved in fracture healing. However, the contributions of such changes do not fully explain the poorer healing outcomes and increased morbidity reported in elderly patients. Future research should address this gap in understanding in order to provide improved and more directed treatment options for the elderly population.
Keywords: Elderly; Fracture healing; Inflamm-aging; Inflammatory response; Senescence.
Conflict of interest statement
Figures
References
-
- Iorio R, Robb WJ, Healy WL, Berry DJ, Hozack WJ, Kyle RF, et al. Orthopaedic surgeon workforce and volume assessment for total hip and knee replacement in the United States: preparing for an epidemic. J Bone Joint Surg Am 2008;90:1598–605. - PubMed
-
- UScensus. U.S. Department of Commerce, Economics and Statistics Administration, U.S. Census Bureau, Washington: 2015. http://www.census.gov/content/dam/Census/library/2015 Accessed 29 July 2015.
-
- Rose S, Maffulli N. Hip fractures: an epidemiological review. Bull Hosp Jt Dis 1999;58:197–201. - PubMed
-
- Green E, Lubahn JD, Evans J. Risk factors, treatment, and outcomes associated with nonunion of the midshaft humerus fracture. J Surg Orthop Adv 2005;14:64–72. - PubMed
-
- Cauley JA, Thompson DE, Ensrud KC, Scott J, Black D. Risk of mortality following clinical fractures. Osteoporos Int 2000;11: 556–61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
