

Comparison of Efficacy and Safety of Liraglutide 3.0 mg in Individuals with BMI above and below 35 kg/m²: A Post-hoc Analysis
- PMID: 29145215
- PMCID: PMC5836203
- DOI: 10.1159/000478099
Comparison of Efficacy and Safety of Liraglutide 3.0 mg in Individuals with BMI above and below 35 kg/m²: A Post-hoc Analysis
Abstract
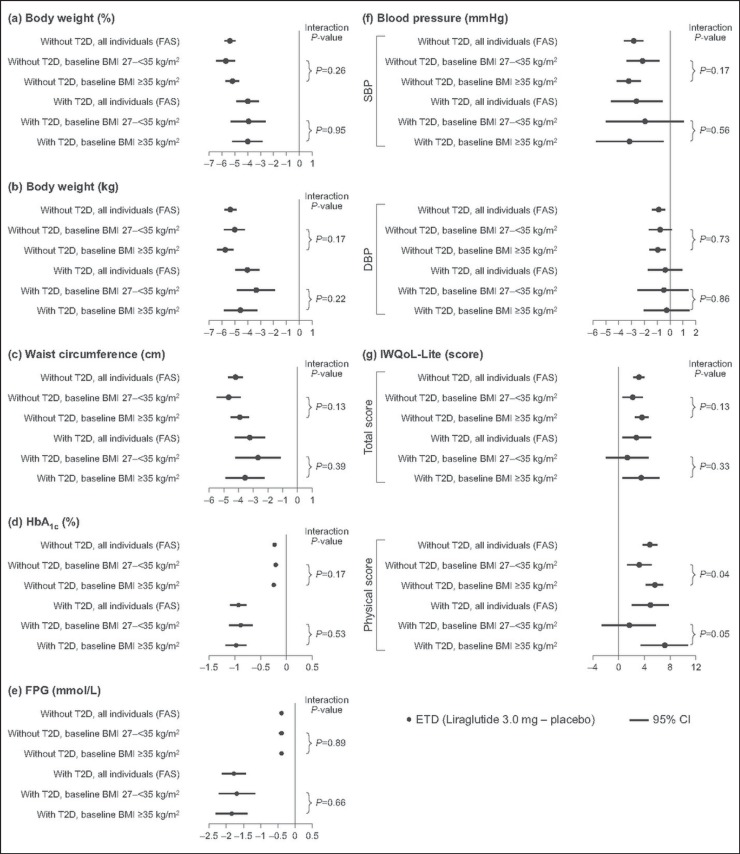
Objective: To investigate whether the efficacy and safety of liraglutide 3.0 mg differed between two subgroups, BMI 27 to <35 and BMI ≥ 35 kg/m², in individuals without and with type 2 diabetes (T2D).
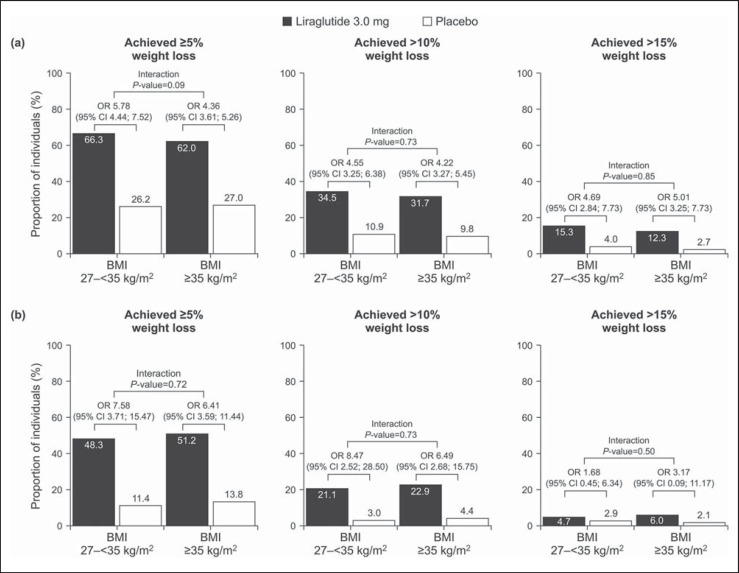
Methods: A post-hoc analysis of two 56-week, randomized, double-blind, placebo-controlled trials (SCALE Obesity and Prediabetes; SCALE Diabetes). Subgroup differences in treatment effects of liraglutide 3.0 mg were evaluated by testing the interaction between treatment group and baseline BMI subgroup.
Results: Significantly greater weight loss (0-56 weeks) was observed with liraglutide 3.0 mg versus placebo in all patient groups while on treatment. There was no evidence that the weight-lowering effect of liraglutide 3.0 mg differed between BMI subgroups (interaction p > 0.05). Similarly, for most secondary endpoints significantly greater improvements were observed with liraglutide 3.0 mg versus placebo, with no indication treatment effects differing between subgroups. The safety profile of liraglutide 3.0 mg was broadly similar across BMI subgroups.
Conclusion: This post-hoc analysis did not indicate any differences in the treatment effects, or safety profile, of liraglutide 3.0 mg for individuals with BMI 27 to <35 or ≥35 kg/m². Liraglutide 3.0 mg can therefore be considered for individuals with a BMI of ≥35 as well as for those with a BMI of 27 to <35 kg/m².
Keywords: Efficacy; Liraglutide; Obesity; Safety.
© 2017 The Author(s) Published by S. Karger GmbH, Freiburg.
Figures
References
-
- Must A, Spadano J, Coakley EH, Field AE, Colditz G, Dietz WH. The disease burden associated with overweight and obesity. JAMA. 1999;282:1523–1529. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
