

Associations between medical cannabis and prescription opioid use in chronic pain patients: A preliminary cohort study
- PMID: 29145417
- PMCID: PMC5690609
- DOI: 10.1371/journal.pone.0187795
Associations between medical cannabis and prescription opioid use in chronic pain patients: A preliminary cohort study
Abstract
Background: Current levels and dangers of opioid use in the U.S. warrant the investigation of harm-reducing treatment alternatives.
Purpose: A preliminary, historical, cohort study was used to examine the association between enrollment in the New Mexico Medical Cannabis Program (MCP) and opioid prescription use.
Methods: Thirty-seven habitual opioid using, chronic pain patients (mean age = 54 years; 54% male; 86% chronic back pain) enrolled in the MCP between 4/1/2010 and 10/3/2015 were compared to 29 non-enrolled patients (mean age = 60 years; 69% male; 100% chronic back pain). We used Prescription Monitoring Program opioid records over a 21 month period (first three months prior to enrollment for the MCP patients) to measure cessation (defined as the absence of opioid prescriptions activity during the last three months of observation) and reduction (calculated in average daily intravenous [IV] morphine dosages). MCP patient-reported benefits and side effects of using cannabis one year after enrollment were also collected.
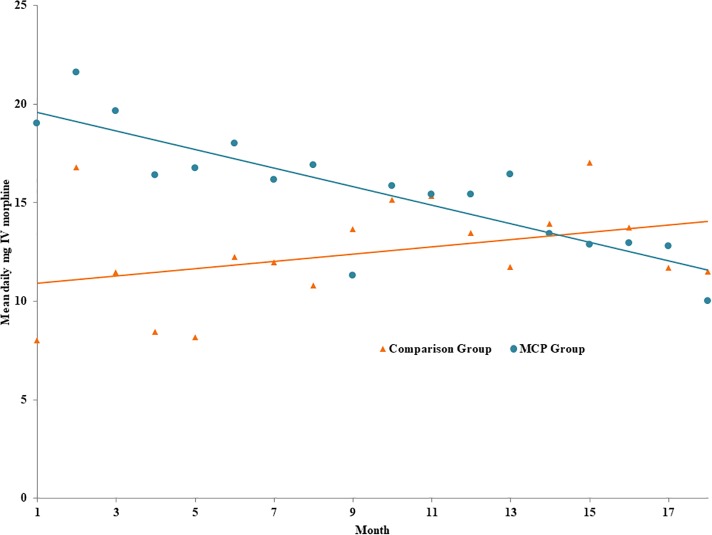
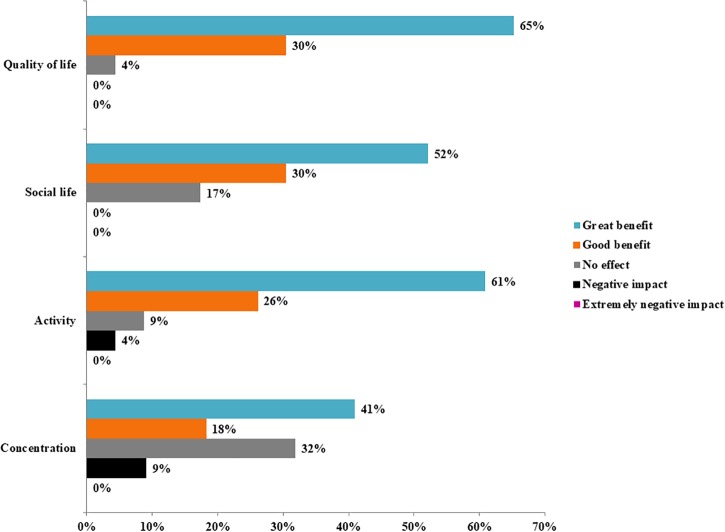
Results: By the end of the 21 month observation period, MCP enrollment was associated with 17.27 higher age- and gender-adjusted odds of ceasing opioid prescriptions (CI 1.89 to 157.36, p = 0.012), 5.12 higher odds of reducing daily prescription opioid dosages (CI 1.56 to 16.88, p = 0.007), and a 47 percentage point reduction in daily opioid dosages relative to a mean change of positive 10.4 percentage points in the comparison group (CI -90.68 to -3.59, p = 0.034). The monthly trend in opioid prescriptions over time was negative among MCP patients (-0.64mg IV morphine, CI -1.10 to -0.18, p = 0.008), but not statistically different from zero in the comparison group (0.18mg IV morphine, CI -0.02 to 0.39, p = 0.081). Survey responses indicated improvements in pain reduction, quality of life, social life, activity levels, and concentration, and few side effects from using cannabis one year after enrollment in the MCP (ps<0.001).
Conclusions: The clinically and statistically significant evidence of an association between MCP enrollment and opioid prescription cessation and reductions and improved quality of life warrants further investigations on cannabis as a potential alternative to prescription opioids for treating chronic pain.
Conflict of interest statement
Figures
References
-
- CDC. Wide-ranging online data for epidemiologic research (WONDER) Atlanta, GA: CDC, National Center for Health Statistics; 2016. Available at http://wonder.cdc.gov.
-
- Rudd RA, Seth P, David F., Scholl L. Increases in drug and opioid-involved overdose deaths—United States, 2010–2015. MMWR Morb Mortal Wkly Rep 2016;65:1445–1452. doi: 10.15585/mmwr.mm655051e1 - DOI - PubMed
-
- Crane EH. Emergency department visits involving buprenorphine. The CBHSQ Report: January 29, 2013. Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, Rockville, MD. - PubMed
-
- Schuckit MA. Treatment of opioid-use disorders. The New England Journal of Medicine, 2016;375:357–368. doi: 10.1056/NEJMra1604339 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
