

Impact of the surgical strategy on the incidence of C5 nerve root palsy in decompressive cervical surgery
- PMID: 29145512
- PMCID: PMC5690695
- DOI: 10.1371/journal.pone.0188338
Impact of the surgical strategy on the incidence of C5 nerve root palsy in decompressive cervical surgery
Abstract
Objective: Our aim was to identify the impact of different surgical strategies on the incidence of C5 palsy.
Background: Degenerative cervical spinal stenosis is a steadily increasing morbidity in the ageing population. Postoperative C5 nerve root palsy is a common complication with severe impact on the patients´ quality of life.
Methods: We identified 1708 consecutive patients who underwent cervical decompression surgery due to degenerative changes. The incidence of C5 palsy and surgical parameters including type and level of surgery were recorded to identify predictors for C5 nerve palsy.
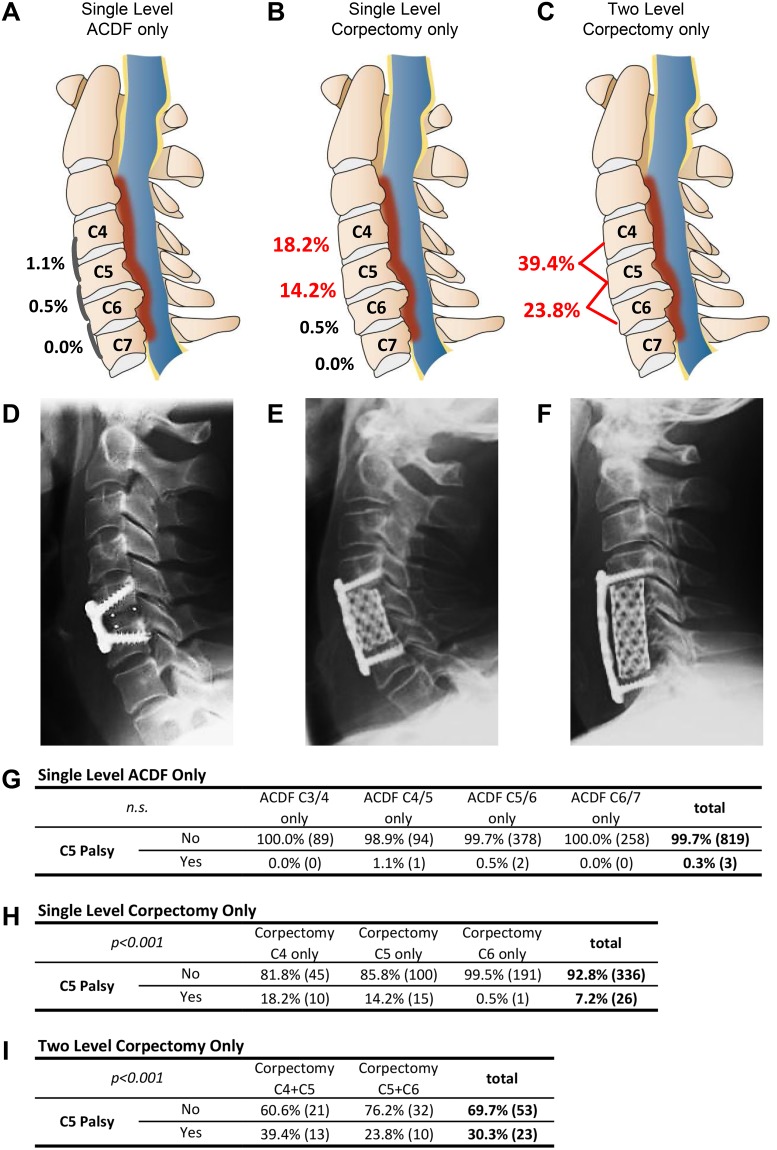
Results: The overall C5 palsy rate was 4.8%, with 18.3% of cases being bilateral. For ACDF alone the palsy rate was low (1.13%), compared to 14.0% of C5 palsy rate after corpectomy. The risk increased with extension of the procedures. Hybrid constructs with corpectomy plus ACDF at C3-6 showed significantly lower rates of C5 palsy (10.7%) than corpectomy of two vertebrae (p = 0.005). Multiple regression analysis identified corpectomy of C4 or C5 as a significant predictor. We observed a lower overall incidence for ventral (4.3%) compared to dorsal (10.9%) approaches (p<0.001). When imaging detected a postoperative shift of the spinal cord at index segment C4/5, palsy rate increased significantly (33.3% vs. 12.5%, p = 0.034).
Conclusions: Extended surgical strategies, such as dorsal laminectomies, multilevel corpectomies and procedures with extensive spinal cord shift were shown to display a high risk of C5 palsy. The use of extended procedures should therefore be employed cautiously. Switching to combined surgical methods like ACDF plus corpectomy can reduce the rate of C5 palsy.
Conflict of interest statement
Figures



Similar articles
-
The incidence of C5 palsy after multilevel cervical decompression procedures: a review of 750 consecutive cases.Spine (Phila Pa 1976). 2012 Feb 1;37(3):174-8. doi: 10.1097/BRS.0b013e318219cfe9. Spine (Phila Pa 1976). 2012. PMID: 22293780 Review.
-
Delayed C5 Palsy After Anterior Cervical Decompression Surgery: Preoperative Foraminal Stenosis and Postoperative Spinal Cord Shift Increase the Risk of Palsy.World Neurosurg. 2018 Dec;120:e1107-e1119. doi: 10.1016/j.wneu.2018.08.240. Epub 2018 Sep 12. World Neurosurg. 2018. PMID: 30218802
-
The association between preoperative spinal cord rotation and postoperative C5 nerve palsy.J Bone Joint Surg Am. 2012 Sep 5;94(17):1605-9. doi: 10.2106/JBJS.K.00664. J Bone Joint Surg Am. 2012. PMID: 22992851
-
Prevalence of C5 nerve root palsy after cervical decompressive surgery: a meta-analysis.Eur Spine J. 2015 Dec;24(12):2724-34. doi: 10.1007/s00586-015-4186-5. Epub 2015 Aug 18. Eur Spine J. 2015. PMID: 26281981
-
C5 nerve root palsy following decompression of cervical spine with anterior versus posterior types of procedures in patients with cervical myelopathy.Eur Spine J. 2016 Jul;25(7):2050-9. doi: 10.1007/s00586-016-4567-4. Epub 2016 Apr 19. Eur Spine J. 2016. PMID: 27095700 Review.
Cited by
-
Intraoperative ultrasonography in laminectomy for degenerative cervical spondylotic myelopathy: a clinical and radiological evaluation.Acta Neurochir (Wien). 2022 Jul;164(7):1873-1881. doi: 10.1007/s00701-022-05232-8. Epub 2022 May 10. Acta Neurochir (Wien). 2022. PMID: 35536511 Free PMC article.
-
A Meta-Analysis of Surgical Outcomes in 25727 Patients Undergoing Anterior Cervical Discectomy and Fusion or Anterior Cervical Corpectomy and Fusion for Cervical Deformity.Global Spine J. 2025 Mar;15(2):1390-1404. doi: 10.1177/21925682241270100. Epub 2024 Aug 1. Global Spine J. 2025. PMID: 39091072 Free PMC article. Review.
-
Surgical options for ossification of the posterior longitudinal ligament of the cervical spine: a narrative review.J Orthop Surg Res. 2024 Nov 1;19(1):707. doi: 10.1186/s13018-024-05215-8. J Orthop Surg Res. 2024. PMID: 39487441 Free PMC article. Review.
-
A systematic review of risk factors and adverse outcomes associated with anterior cervical discectomy and fusion surgery over the past decade.J Craniovertebr Junction Spine. 2024 Apr-Jun;15(2):141-152. doi: 10.4103/jcvjs.jcvjs_168_23. Epub 2024 May 24. J Craniovertebr Junction Spine. 2024. PMID: 38957769 Free PMC article. Review.
-
C5 Nerve Palsy After Posterior Instrumentation and Decompression in Cervical Spine Surgery: A Review of the Literature.Cureus. 2025 May 19;17(5):e84430. doi: 10.7759/cureus.84430. eCollection 2025 May. Cureus. 2025. PMID: 40539182 Free PMC article. Review.
References
-
- Shou F, Li Z, Wang H, Yan C, Liu Q, Xiao C. Prevalence of C5 nerve root palsy after cervical decompressive surgery: a meta-analysis. Eur Spine J. 2015;24: 2724–34. doi: 10.1007/s00586-015-4186-5 - DOI - PubMed
-
- Guzman JZ, Baird EO, Fields AC, McAnany SJ, Qureshi SA, Hecht AC, et al. C5 nerve root palsy following decompression of the cervical spine: a systematic evaluation of the literature. Bone Joint J. 2014;96–B: 950–5. doi: 10.1302/0301-620X.96B7.33665 - DOI - PubMed
-
- Sakaura H, Hosono N, Mukai Y, Ishii T, Yoshikawa H. C5 palsy after decompression surgery for cervical myelopathy: review of the literature. Spine (Phila Pa 1976). 2003;28: 2447–51. doi: 10.1097/01.BRS.0000090833.96168.3F - DOI - PubMed
-
- Katsumi K, Yamazaki A, Watanabe K, Ohashi M, Shoji H. Can prophylactic bilateral C4/C5 foraminotomy prevent postoperative C5 palsy after open-door laminoplasty? A prospective study. Spine (Phila Pa 1976). 2012;37: 748–54. doi: 10.1097/BRS.0b013e3182326957 - DOI - PubMed
-
- Currier BL. Neurological complications of cervical spine surgery: C5 palsy and intraoperative monitoring. Spine (Phila Pa 1976). 2012;37: E328–34. doi: 10.1097/BRS.0b013e3182417276 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
