

Preconceptual Zika virus asymptomatic infection protects against secondary prenatal infection
- PMID: 29145516
- PMCID: PMC5689831
- DOI: 10.1371/journal.ppat.1006684
Preconceptual Zika virus asymptomatic infection protects against secondary prenatal infection
Abstract
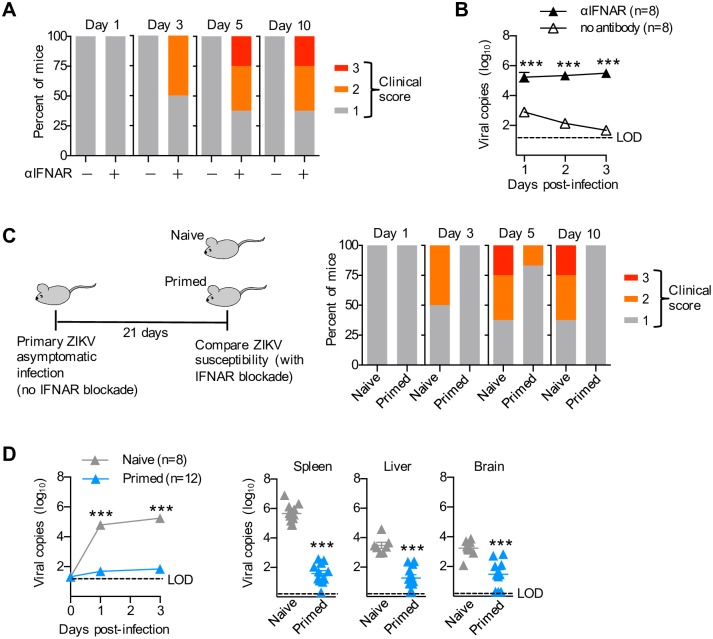
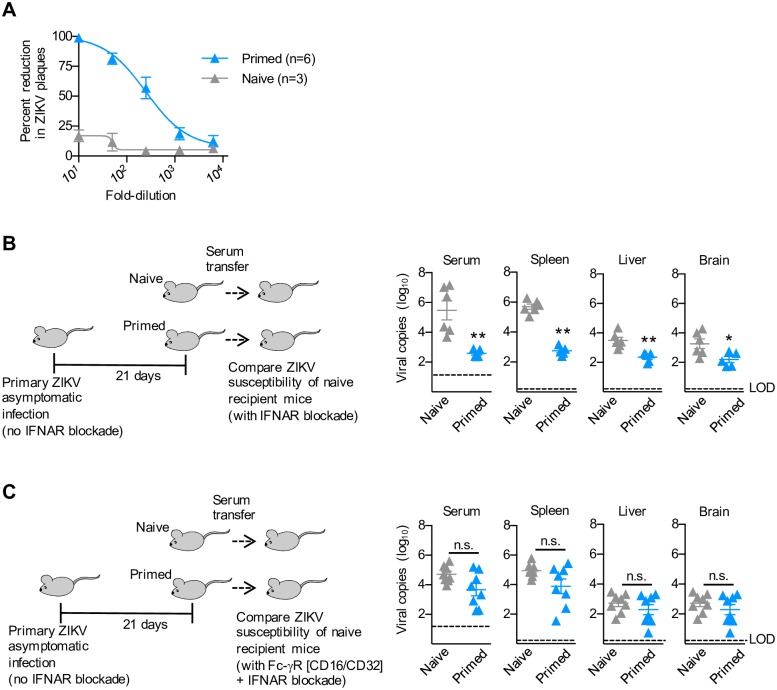
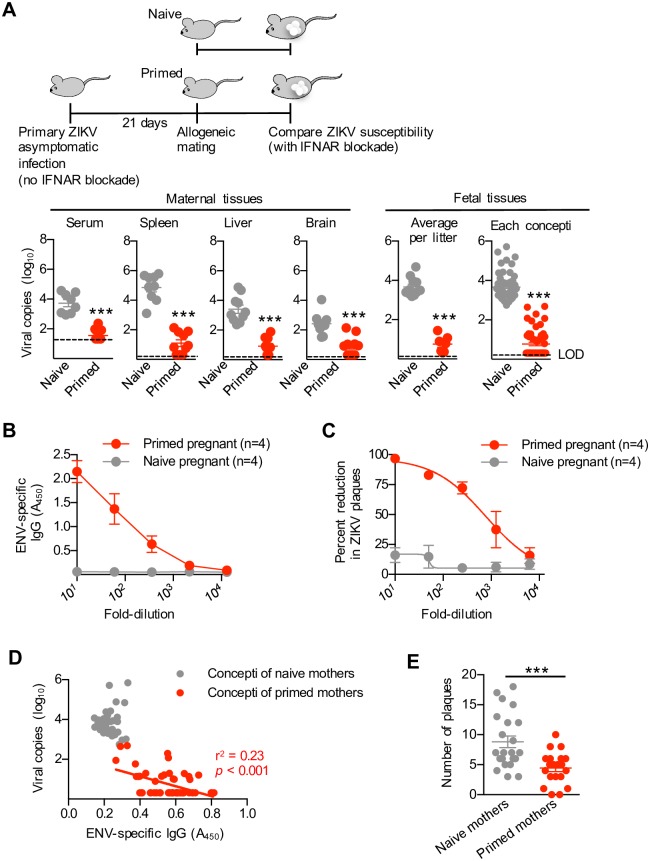
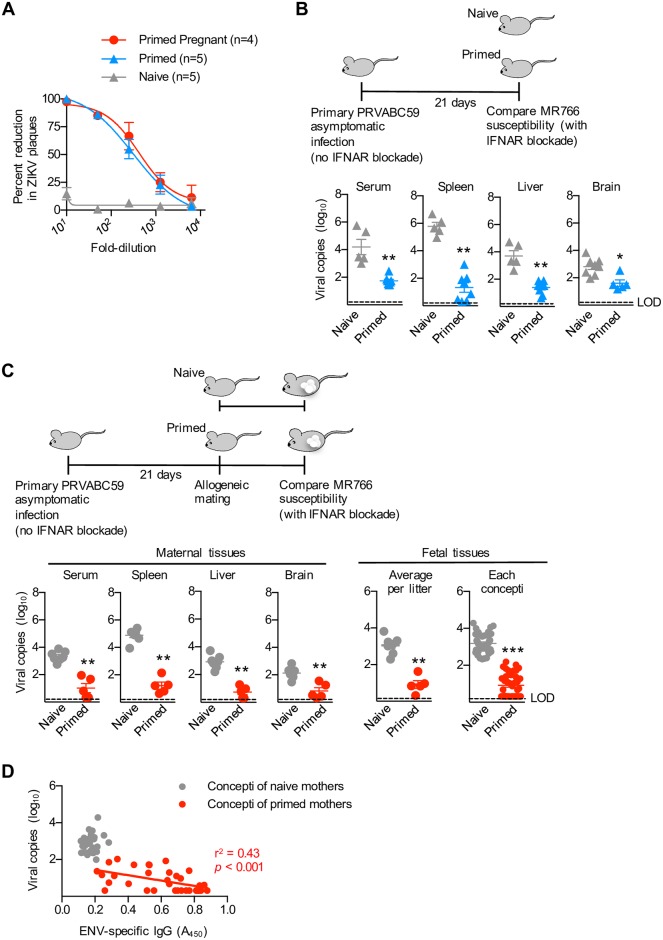
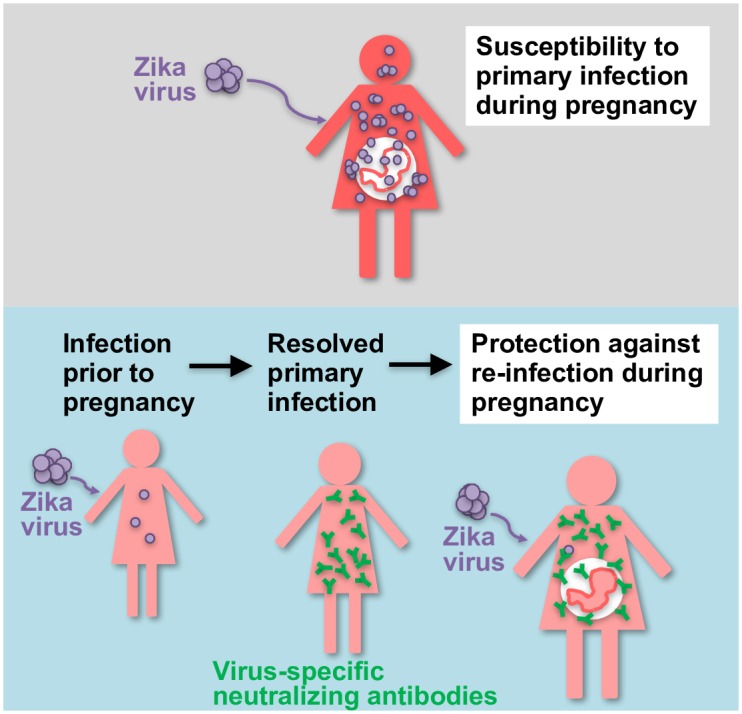
Pregnant women, and their fetal offspring, are uniquely susceptible to Zika virus and other microbial pathogens capable of congenital fetal infection. Unavoidable exposure to Zika virus in endemic areas underscores the need for identifying at-risk individuals, and protecting expecting mothers and their fetal offspring against prenatal infection. Here we show that primary Zika virus asymptomatic infection in mice confers protection against re-infection, and that these protective benefits are maintained during pregnancy. Zika virus recovery was sharply reduced in maternal tissues and amongst fetal concepti after prenatal challenge in mothers with resolved subclinical infection prior to pregnancy compared with mice undergoing primary prenatal infection. These benefits coincide with expanded accumulation of viral-specific antibodies in maternal serum and fetal tissues that protect against infection by the identical or heterologous Zika virus genotype strains. Thus, preconceptual infection primes Zika virus-specific antibodies that confer cross-genotype protection against re-infection during pregnancy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Fauci AS, Morens DM. Zika Virus in the Americas—Yet Another Arbovirus Threat. N Engl J Med. 2016;374(7):601–4. doi: 10.1056/NEJMp1600297 . - DOI - PubMed
-
- Lazear HM, Diamond MS. Zika Virus: New Clinical Syndromes and Its Emergence in the Western Hemisphere. J Virol. 2016;90(10):4864–75. doi: 10.1128/JVI.00252-16 - DOI - PMC - PubMed
-
- Coyne CB, Lazear HM. Zika virus—reigniting the TORCH. Nat Rev Microbiol. 2016;14(11):707–15. doi: 10.1038/nrmicro.2016.125 . - DOI - PubMed
-
- Miner JJ, Diamond MS. Zika Virus Pathogenesis and Tissue Tropism. Cell Host Microbe. 2017;21(2):134–42. doi: 10.1016/j.chom.2017.01.004 - DOI - PMC - PubMed
-
- Brasil P, Pereira JP Jr., Moreira ME, Ribeiro Nogueira RM, Damasceno L, Wakimoto M, et al. Zika Virus Infection in Pregnant Women in Rio de Janeiro. N Engl J Med. 2016;375(24):2321–34. doi: 10.1056/NEJMoa1602412 . - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
