

The Changing Paradigm of Management of Liver Abscesses in Chronic Granulomatous Disease
- PMID: 29145578
- PMCID: PMC6248449
- DOI: 10.1093/cid/cix1012
The Changing Paradigm of Management of Liver Abscesses in Chronic Granulomatous Disease
Abstract
Background: Chronic granulomatous disease (CGD) is a rare genetic disorder causing recurrent infections. More than one-quarter of patients develop hepatic abscesses and liver dysfunction. Recent reports suggest that disease-modifying treatment with corticosteroids is effective for these abscesses. Comparison of corticosteroid therapy to traditional invasive treatments has not been performed.
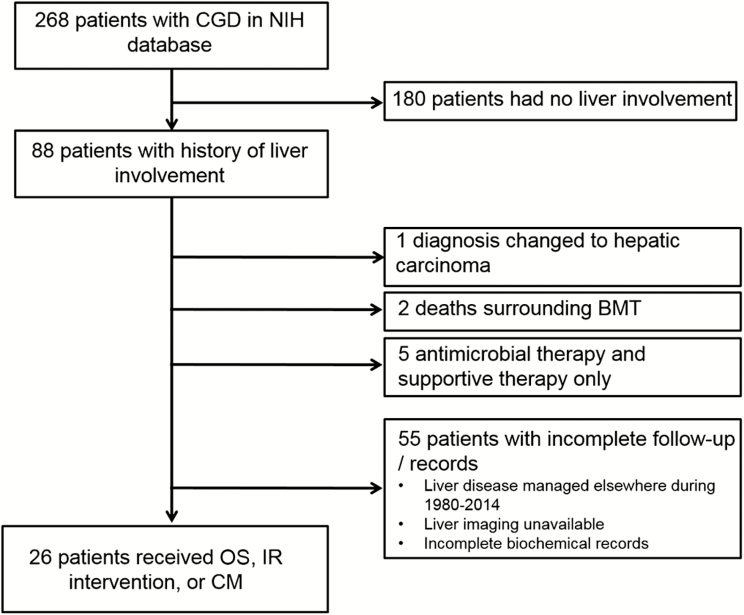
Methods: Records of 268 patients with CGD treated at the National Institutes of Health from 1980 to 2014 were reviewed. Patients with liver involvement and complete records were included. We recorded residual reactive oxygen intermediate (ROI) production by neutrophils, nicotinamide adenine dinucleotide phosphate (NADPH) oxidase germline mutation status, laboratory values, imaging characteristics, time to repeat hepatic interventions, and overall survival among 3 treatment cohorts: open liver surgery (OS), percutaneous liver-directed interventional radiology therapy (IR), and high-dose corticosteroid management (CM).
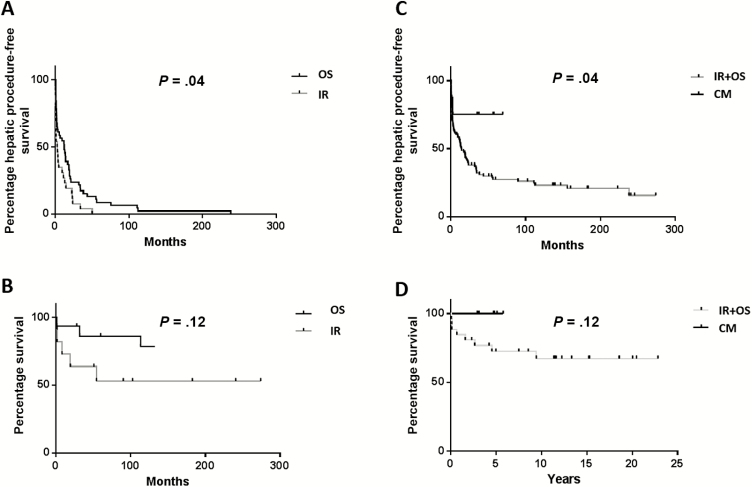
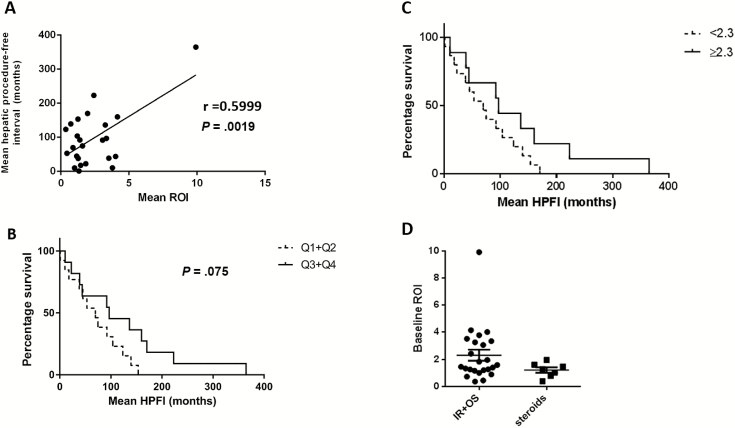
Results: Eighty-eight of 268 patients with CGD suffered liver involvement. Twenty-six patients with a median follow-up of 15.5 years (8.5-32.9 years of follow-up) had complete records and underwent 100 standard interventions (42 IR and 58 OS). Eight patients received a treatment with high-dose corticosteroids only. There were no differences in NADPH genotype, size, or number of abscesses between patients treated with OS, IR, or CM. Time to repeat intervention was extended in OS compared with IR (18.8 vs 9.5 months, P = .04) and further increased in CM alone (median time to recurrence not met). Impaired macrophage and neutrophil function measured by ROI production correlated with shorter time to repeat intervention (r = 0.6, P = .0019).
Conclusions: Treatment of CGD-associated liver abscesses with corticosteroids was associated with fewer subsequent hepatic interventions and improved outcome compared to invasive treatments.
Figures
References
-
- Winkelstein JA, Marino MC, Johnston RB Jr et al. Chronic granulomatous disease. Report on a national registry of 368 patients. Medicine (Baltimore) 2000; 79:155–69. - PubMed
-
- Segal BH, Leto TL, Gallin JI, Malech HL, Holland SM. Genetic, biochemical, and clinical features of chronic granulomatous disease. Medicine (Baltimore) 2000; 79:170–200. - PubMed
-
- Hussain N, Feld JJ, Kleiner DE et al. Hepatic abnormalities in patients with chronic granulomatous disease. Hepatology 2007; 45:675–83. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
