

Risk factors associated with the progression and metastases of hindgut neuroendocrine tumors: a retrospective study
- PMID: 29145818
- PMCID: PMC5693490
- DOI: 10.1186/s12885-017-3769-4
Risk factors associated with the progression and metastases of hindgut neuroendocrine tumors: a retrospective study
Abstract
Background: The worldwide incidence of neuroendocrine tumors (NETs) has increased remarkably, with the hindgut being the second most common site for such tumors. However, the mechanisms underlying progression and metastasis of hindgut NETs are unclear. A retrospective study was conducted to elucidate these mechanisms.
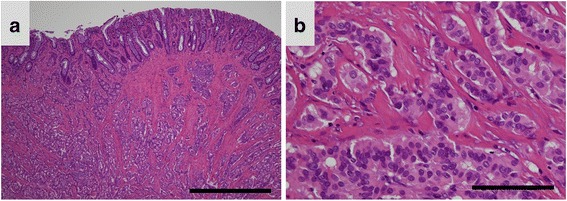
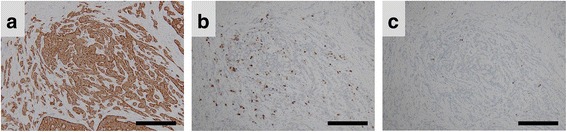
Methods: Clinicopathological data of cases of hindgut NET between April 1996 and September 2015 were analyzed, retrospectively. Patients with neuroendocrine carcinoma were excluded. Formalin-fixed paraffin-embedded tissues of hindgut NET cases were subjected to detailed morphometric and immunohistochemical analyses. Statistical analyses were performed using the non-parametric Mann-Whitney U test, Spearman's correlation coefficient, and chi-squared test. Multivariate logistic regression analysis was conducted as appropriate for the data set.
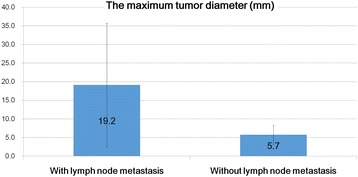
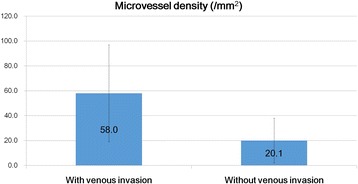
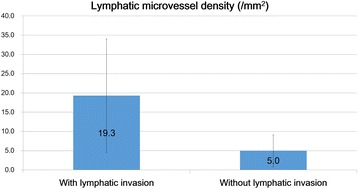
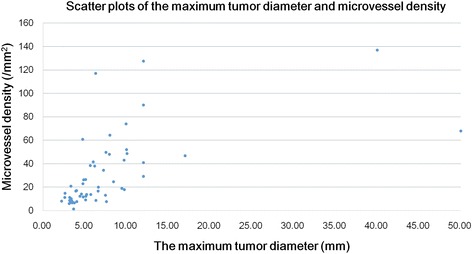
Results: Fifty-six hindgut NET cases were considered. Microvessel density and lymphatic microvessel density were identified as significant risk factors for venous and lymphatic invasion. There was a positive correlation between microvessel density and the maximum tumor diameter. Multivariate logistic regression analysis revealed that the maximum tumor diameter alone was an independent predictor of lymph node metastasis, whereas lymphovascular invasion and MVD was not the predictor of lymph node metastasis. There were no significant correlations between the Ki-67 labeling index and any of the parameters evaluated including age, sex, the maximum tumor diameter, venous invasion, lymphatic invasion, microvessel density, lymphatic microvessel density, and lymph node metastasis.
Conclusions: Angiogenic mechanisms may play important roles in the progression of hindgut NET. Otherwise, the maximum tumor diameter alone was an independent predictor of lymph node metastasis in hindgut NETs. Moreover, our study raises the question of whether the presence of lymphovascular invasion, in endoscopically obtained hindgut NET tissues, is an absolute indication for additional surgery or not.
Keywords: Angiogenesis; Hindgut; Lymphatic microvessel density; Lymphovascular invasion; Microvessel density; Neuroendocrine tumor.
Conflict of interest statement
Ethics approval and consent participate
This retrospective study was performed in accordance with the Declaration of Helsinki and approved by the Ethics Review Committee of Kanagawa Cancer Center, Kanagawa, Japan (Approval Number: 27–38). Furthermore, written informed consent was obtained at the time of clinical intervention for the future use of material for research in all cases.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Sevilla I, Segura A, Capdevila J, Lopez C, Garcia-Carbonero R, Grande E, et al. Management of controversial gastroenteropancreatic neuroendocrine tumour clinical situations with somatostatin analogues: results of a Delphi questionnaire panel from the NETPraxis program. BMC Cancer. 2016;16:858. doi: 10.1186/s12885-016-2901-1. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
